
Download
REVIEW ARTICLE
Cardiac arrhythmia and immune response in COVID-19 patients
Chunlian Wanga, Wenqiang Haob*
aInstitute for Prevention and Control of Chronic Non-communicable Diseases, Harbin Center for Disease Control and Prevention, Harbin, China
bThe Second Ward of Internal Medicine, The Second Hospital of Heilongjiang Province, Harbin, China
Abstract
The coronavirus disease 2019 (COVID-19) pandemic has presented substantial challenges for providing health care due to the numerous complications on the respiratory and cardiovascular systems of people. Cardiac arrhythmia is one of the cardiac complications, and it was observed in COVID-19 patients. Moreover, arrhythmia and cardiac arrest are common in COVID-19 patients in the intensive care unit. The occurrence of cardiac arrhythmia in COVID-19 patients is associated with hypoxia, cytokine storm, myocardial ischemia and inflammatory disease such as congestive heart failure. It is necessary to know the occurrence and mechanisms of tachyarrhythmia and bradyarrhythmia in patients with COVID-19 infection for their proper management. This review provides an overview of the association between COVID-19 and arrhythmias by detailing possible pathophysiological mechanisms.
Key words: heart diseases, SARS-Cov2, arrhythmia, Immune response, Cytokine
*Corresponding author: Wenqiang Hao, The Second Ward of Internal Medicine, The Second Hospital of Heilongjiang Province, Harbin, Heilongjiang Province, China. Email addresses: [email protected]; [email protected]
Received 30 March 2023; Accepted 15 April 2023; Available online 1 July 2023
Copyright: Wang C, et al.
License: This open access article is licensed under Creative Commons Attribution 4.0 International (CC BY 4.0). http://creativecommons.org/licenses/by/4.0/
Introduction
The main cause of human mortality is cardiovascular diseases (CVD), which accounted for 31% of global deaths in 2016.1 Arrhythmia can be mentioned among the most important heart diseases. Cardiac arrhythmia or disturbance in the heart rhythm is usually caused by improper functioning of the electrical messages coordinating the heart rate and leads to an increase or decrease in the rate or its irregularity. Cardiac arrhythmias may be described as heart palpitations, which are sometimes harmless. However, some arrhythmias may be associated with distressing and sometimes fatal signs and symptoms. Arrhythmias can be a Bradyarrhythmia (<60 beats per minute) or a Tachyarrhythmia (>100 beats per minute) and can occur at any age.2
Various factors can affect the normal cardiac rhythm and cause arrhythmia. Genetic causes and acquired causes are mentioned. Genetic causes can include channelopathies (Brugada syndrome, Catecholaminergic Polymorphic Ventricular Tachycardia, short and long QT syndrome [LQTS]) or congenital structural disorders (Tetralogy of Fallot, Transposition of the great arteries, and Ebstian syndrome). Acquired causes can include a wide range of related factors, such as electrolyte imbalance (such as -calcium-, potassium-, and magnesium-level changes), myocardial damage (such as myocarditis, cardiac ischemia), body temperature changes (fever, hypothermia), infections, remodeling of the heart structure (hypertrophic cardiomyopathy, dilated cardiomyopathy, and restrictive cardiomyopathy), and acquired valvular disease.3
The COVID-19 is the greatest challenge of the century, which has led to huge health costs worldwide to fight this global pandemic and healthcare services.4 Severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2), which causes COVID-19, was first reported in China on December 31, 20195 and COVID-19 has been introduced as a pandemic with far-reaching effects on the health and economic sectors of the world.6
Cardiovascular complications are one of the most important complications of COVID-19 infection. In a recent series of cases published from New York, various types of atrial and ventricular tachyarrhythmias and bradyarrhythmias have been reported in patients infected with coronavirus.7 One of the most important aspects of cardiac injury is the increased risk of cardiac arrhythmias, so in this review, we present the current state of knowledge regarding the potential mechanisms and manifestations of cardiac arrhythmia in patients with COVID-19 as a resource for clinicians during this rapidly evolving crisis.
Tachyarrhythmia
In normal body conditions, more than 100 beats per minute presents tachyarrhythmia that can occur at any age. Tachyarrhythmia is divided into two general groups based on the place where it originates: tachyarrhythmia with ventricular origin and tachyarrhythmia with atrial origin. Arrhythmias originating from the ventricles are divided into several major groups including: (1) anatomical reentry around an obstacle such as a scar manifesting as monomorphic ventricular tachycardia (MMVT), (2) functional re-entry due to a stable rotor, which also manifests as monomorphic VT (MM VT), (3) re-entry due to a tortuous rotor seen as polymorphic VT (PMVT) or Torsade’s de Point (TDP), (4) multiple wavelet ventricular fibrillation (VF) due to rotor (spiral/scroll wave) breakup, (5) mother rotor ventricular fibrillation (VF) due to a fast stable rotor with peripheral wave breaks (fibrillary conduction block) in surrounding tissue, and (6) ventricular flutter (VFL). When electrical signals in the ventricles are released too quickly and without control, ventricular fibrillation occurs, which causes the lower chambers to vibrate, so the heart cannot pump blood. If the person is not treated immediately and a normal rhythm is not established quickly, the person will suffer brain and heart damage and die, and (7) premature ventricular contraction (PVC). An electrical signal from the ventricles causes a premature heartbeat that is usually ignored. These beats are usually seen in both healthy and sick people.8
Ventricular arrhythmias may be nonsustained or sustained, e.g. non-SUS-VT or SUS VT), may be triggered or focally or completely reentrant in origin, or involved in combination of focal and reentrant mechanisms.9 In addition, sometimes reentrant circuits, which are not intrinsically stable, can be constantly re-triggered by focal activations and persist (mixed focal reentrant-VF).9
On the other hand, important ventricular arrhythmias can be divided into three general categories from another point of view, in which primary dynamic instability causes dysrhythmias: (1) Decreased repolarization includes LQTS and HF; Arrhythmia manifestations in the group are TDP & PVT and mixed reentrant-focal VF, (2) additional repolarization includes ischemia, BS, ERS, SQTS; arrhythmia manifestations in the group are multiple wavelet VF and mother rotor VF, and (3) unstable calcium cycle includes CPVT, HF, and ischemia arrhythmia manifestations in the group are DAD-mediated VT, Multiple wavelet VF, and mother rotor VF.10
Arrhythmias originating from the atrial are divided into several groups including; (1) sinus tachycardia: sinus tachycardia occurs when the heartbeat originates from the sinus node, but the heart rate exceeds 100, (2) atrial fibrillation (AF): AF occurs when action potentials are fired too rapidly within the atria at different points, leading to a rapid increase in atrial rate (approximately 0–40–60 beats per minute). Due to the very high speed of the atrium, P waves may not be seen. Conduction from the atrium to the ventricle has changed; therefore, in addition to the irregularity of the atrial rhythm, the ventricular rhythm is also irregular, (3) premature atrial contraction (PAC): PAC causes the regular heart rhythm to be interrupted with a premature beat. This premature beat is often generated from the atria and from a place outside the sinus node, (4) aberrant beats of atrial rhythm (AT): This rhythm occurs when a place outside the sinus node in the atria temporarily takes over the task of pacing the heart because it creates an action potential faster than the sinus, atrial tachycardia can be focal. That is, all the bits originate from a fixed place (AT). And sometimes, atrial tachycardia is multifocal (MAT), (5) atrial flutter (AFL): AFL is a prevalent abnormal heart rhythm that starts in the atrial chambers of the heart. When it first occurs, it is usually associated with a fast heart rate and is classified as a type of supraventricular tachycardia (SVT), and (6) SVT: SVT is fast heart rate staring in the upper heart chambers. The mechanism of supraventricular arrhythmia is the presence of reentry circuits and has a wide division that is beyond the scope of this study.10
Bradyarrhythmia
Bradyarrhythmias can be due to dysfunction of the sinoatrial node (SAN) and sometimes due to block in the atrioventricular node (AVN) and His-Purkinje system (HPs). Therefore, they are divided depending on the place where the function is disturbed, including (1) sinus bradycardia: The beats originate from the SAN, but the pulse rate is less than normal (<60), (2) sick sinus syndrome: The sinus tract does not release its signals well, which makes the heartbeat irregular. Sometimes the heart rate varies between bradycardia and tachycardia. This type of heart rhythm is seen in elderly people as a result of a generational change in the conduction path of the heart, (3) first class AVN block. This is when the conduction of the atrium to the ventricle is carried out in a 1:1, but at the site of the AVN, there is a delay in the conduction, and therefore, it is seen in the ECG as an increase in the PR interval, (4) Mobitz I (Wenckbach) Narrow QRS, progressive increase in PR interval until one ventricular beat is eliminated, then this process repeats, (5) Mobitz II fixed PR interval with beats that are occasionally removed with a 2-to-1, 3-to-1, and 4-to-1 scheme; The QRS complex is usually wide, seen with MI or degenerative diseases of the conduction system; This rhythm is dangerous and may suddenly progress to complete atrial-ventricular block, and (6) third degree (complete atrial-ventricular block) the activity of the atria is transferred to the ventricles and in this type, atria and ventricles can have independently contraction (Table 1).11,12
Table 1 Arrhythmia classification.
| Tachyarrhythmia | Atrial | Sinus tachycardia |
| Atrial fibrillation (AF) | ||
| Premature atrial contraction (PAC) | ||
| Aberrant beats of atrial rhythm (AT) | ||
| Atrial flutter (AFL) | ||
| Supraventricular tachycardia (SVT) | ||
| Ventricular | Anatomical reentry around an obstacle such as a scar manifesting as monomorphic ventricular tachycardia (MMVT) | |
| Functional re-entry due to a stable rotor, which also manifests as monomorphic VT (MM VT) | ||
| Re-entry due to a tortuous rotor seen as polymorphic VT (PMVT) or Torsade’s de Point (TDP) | ||
| Multiple wavelet ventricular fibrillation (VF) due to rotor (spiral/scroll wave) breakup | ||
| Mother rotor ventricular fibrillation (VF) due to a fast stable rotor with peripheral wave breaks (fibrillary conduction block) in surrounding tissue | ||
| Ventricular flutter (VFL). When electrical signals in the ventricles are released too quickly and without control, ventricular fibrillation occurs. It causes the lower chambers to vibrate, so the heart cannot pump blood. If the person is not treated immediately and a normal rhythm is not established quickly, the person suffers brain and heart damage and dies | ||
| Premature ventricular contraction (PVC). An electrical signal from the ventricles causes a premature heartbeat that is usually ignored. These beats are usually seen in both healthy and sick people | ||
| Bradyarrhythmia | Sinus bradycardia | |
| Sick sinus syndrome | ||
| First class atrioventricular node (AVN) block | ||
| Mobitz I | ||
| Mobitz II | ||
| Complete heart block | ||
Arrhythmia and COVID-19 Infection
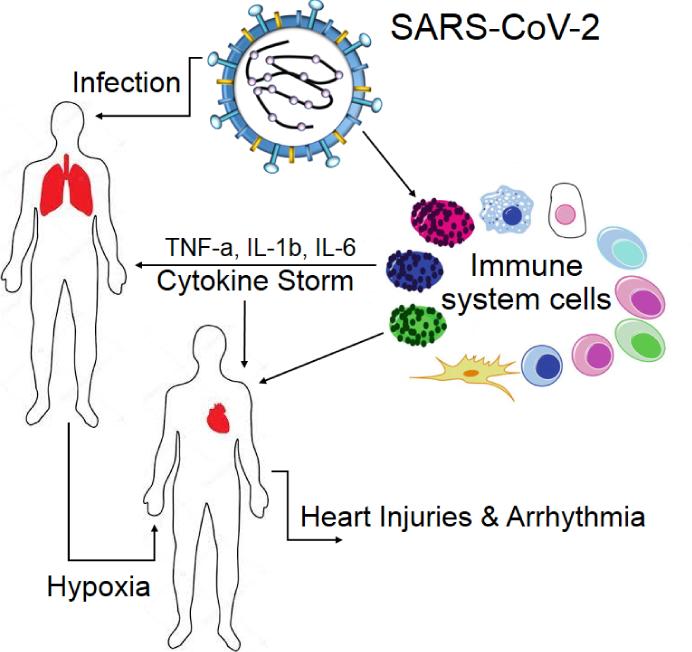
SARS-CoV-2 is the cause of coronavirus disease 2019 (Covid-19), and this viral disease has easily spread all over the world and has become an epidemic.5,13,14 The most common symptoms include fever, cough, and fatigue. Few patients experience complications such as acute respiratory distress syndrome (ARDS) and other end-organ damage.15 Although the most common and prominent symptoms in most patients infected with COVID-19 are respiratory symptoms, many studies reported extra pulmonary involvement, including the cardiovascular system (Figure 1).16,17 In a study, it was mentioned that the mortality rate of COVID-19 people who suffering from cardiac complications was 51.2%, while the mortality rate was 4.5% in the absence of cardiac complications.17,18 Similarly, in another study, the presence of cardiac injury was associated with fatal outcomes, with a significantly higher mortality of 59.6% compared to patients without cardiac injury (8.9%).19 In a study, it was shown that cardiac arrhythmia occurs in 6 to 17% of patients.20 However, it increases to 44% in patients admitted to the intensive care unit (ICU), and the second most common complication after ARDS is cardiac arrhythmia.20 Types of tachycardia including AF, AFL, SVT, and ventricular arrhythmia have been reported in patients with COVID-19.21 The occurrence of cardiac arrhythmias following infection with the COVID-19 virus is a multifactorial phenomenon.22
Figure 1 Related immune response in the effect of COVID-19 on the respiratory and cardiovascular systems.
The most common arrhythmia that was observed in COVID-19 patients is supraventricular arrhythmia, and among them, AF is the most common arrhythmia that occurs in about 15–30% of them. Unfortunately, the occurrence of AF in patients infected with COVID-19 causes an increase in severe clinical manifestations.23 Various mechanisms are involved in the occurrence of AF.24 Among its causes, the following can be mentioned: the presence of hypoxemia following pulmonary involvement can cause heart damage and primyocarditis, in which AF may occur; the common occurrence of COVID-19 infection in older patients who are already susceptible to suffering from AF can be another cause.25 Another common rhythm disorder in patients with COVID-19 is sinus tachycardia due to several reasons including respiratory failure/hypoxemia, fever, hemodynamic disorder, pain, and fear/anxiety.26 Sinus bradycardia can also be a manifestation of COVID-19 infection and is a reason for careful monitoring of patients. The occurrence of sinus bradycardia has various reasons, including inflammatory damage to the sinus node by circulating cytokines, severe hypoxia, and side effects of drugs. Sinus bradycardia can be a sign of the beginning of a serious cytokine storm.27
In case of damage to the myocardium and myocardial ischemia (MI) or acute myocarditis, the person becomes prone to various and serious ventricular arrhythmias.28 Ventricular tachyarrhythmias can occur in different conditions and even endanger a person’s life. It occurs in conditions such as myocarditis, ischemic heart disease (IHD), chronic heart failure (CHF), and other heart muscle conditions. Ischemic heart disease is responsible for approximately 65% of sudden cardiac death (SCD) cases, while the remainder is associated with structural heart diseases [arrhythmogenic right ventricular cardiomyopathy (ARVC), hypertrophic cardiomyopathy, valvular heart disease, myocarditis] and pre-arrhythmic diseases (long QT, short QT, Brugada, and pre-excitation syndromes, respectively).29 In case of damage to the myocardium and MI or acute myocarditis, the person becomes prone to various and serious ventricular arrhythmias.30 In addition to this, there are other triggers for the occurrence of ventricular arrhythmia in these patients, which include severe respiratory failure and resulting hypoxia, systemic inflammation and cytokine storm, autonomic imbalance, electrolyte disorders, and pre-arrhythmic complications of COVID-19 treatments and drug interactions.31 Patients with severe cases of COVID-19 often have other co-morbidities that can increase the risk of developing malignant VAs, such as fever, electrolyte abnormalities (hypokalemia, hypomagnesemia), a history of underlying heart disease, and most importantly, drug treatments for COVID-19, which can be proarrhythmic and cause QT prolongation, and as a result, may cause TDP and SCD.32 Also, acute myocardial injury caused by a virus can independently cause QT interval prolongation.30 In a case series of 121 patients diagnosed with COVID-19 infection, 71.9% were found to have tachycardia independent of hypotension and fever, and 14.9% were found to have transient bradyarrhythmia. Tachycardia persisted in 40% of patients after discharge.33 In a case series of 137 patients with coronavirus, nearly 7.3% reported palpitations as the initial symptom.34 In another, 16.7% of patients with COVID-19 infection had arrhythmias, with a higher incidence of 44.4% in ICU patients compared to non-ICU patients.20 There was low prevalence of arrhythmia among patients with COVID-19 with clinical stability.35 A case series by Guo et al. reported a 5.9% incidence of sustained episodes of ventricular tachycardia or ventricular fibrillation in 187 hospitalized COVID-19 patients.19 In a case series of 70 patients with COVID-19, cardiac arrhythmias including tachyarrhythmia and severe bradyarrhythmia requiring temporary pacemaker occurred in 15.7% of patients.36
Several manifestations of arrhythmia have been observed in COVID-19 patients and bradyarrhythmia has been described in several literatures. Bradycardia, including sinus or AV block, can occur in patients with COVID-19. There are various reasons for the occurrence of bradyarrhythmias in COVID-19 patients, such as side effects of drugs like azithromycin, hydroxyl chloroquine, and lopinavir/rotinavir. In myocarditis, it is also possible to involve the conduction system, especially AV blocks. Also, in intubated patients, transient bradycardia may occur during suctioning of tracheal secretions due to transient increase in vagal tone.37
Cases of complete heart block have been reported in a patient with COVID-19.38 Also, we reported a case of permanent atrioventricular (AV) block in one of our patients, which ultimately required the implantation of a permanent micro cardiogram.11 Another case of high-grade transient AV block following subclinical myocarditis in a patient infected with coronavirus was reported.39 In a recent series of cases published from New York, various types of atrial and ventricular tachyarrhythmias and bradyarrhythmias have been reported in patients infected with coronavirus.7
There are several mechanisms for the cardiac arrhythmia occurrence during the infection of COVID-19; including various conditions of damage to the myocardium such as myocardial infarction, myocarditis, and severe systolic heart failure.40 In the conditions of a viral infection, chronic CVDs can become unstable due to the increase in metabolic demand and provide basis for the occurrence of various types of arrhythmia.40 This imbalance of supply and demand, in association with direct myocardial damage and increased inflammatory response, can increase the risk of acute coronary syndrome, acute heart failure, and cardiac arrhythmia.41,42 COVID-19 infection can cause hypoxia by directly affecting the lung tissue, and following hypoxia, myocardial involvement causes arrhythmia.22 Hypoxia can activate anaerobic glycolysis, and therefore cause acidosis inside the heart cells, and as a result, the function of hydrogen/sodium channels is affected and hydrogen exits the cell at the expense of entering large amounts of sodium. Then, the intracellular sodium causes the sodium–calcium exchange channels to enter into action and, with the sodium deficit, enter large amounts of calcium into the cell and increase the cytosolic calcium level. An increase in the intracellular calcium level can facilitate early and late depolarization, as well as changes in the duration of the action potential, and therefore provide the basis for the occurrence of various types of cardiac arrhythmias.43 Hypoxia also increases the extracellular potassium level, which lowers the depolarization threshold and accelerates electrical conduction. This can also be the reason for the occurrence of arrhythmia.44 In addition, hypoxemia can also reduce electrical coupling and tissue anisotropy due to dephosphorylation of connexin 43 at gap junctions.45
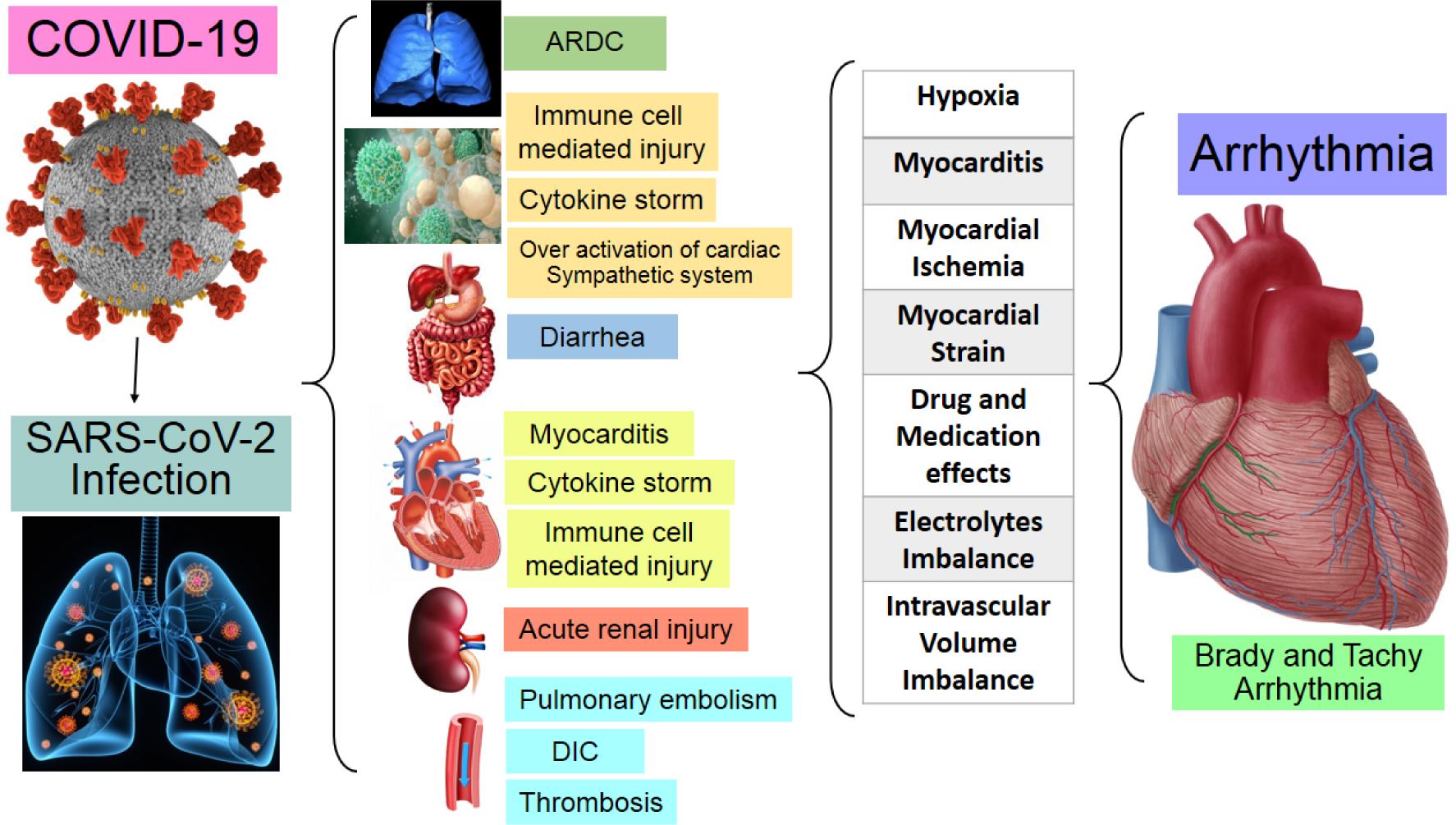
On the other hand, stimulating the response of the immune system to deal with this infection can cause the disruption of cytokines and the storm of cytokines can cause damage to the heart tissue or trigger the occurrence of arrhythmia (Figure 2).22 In the damage to the myocardium following COVID-19 infection, some cytokines play a prominent role and can be a trigger for the occurrence of arrhythmia.46 Among them, interleukin (IL)-6, tumor necrosis factor (TNF)-α, and IL-1 can affect the expression and function of potassium and calcium channels and prolong the ventricular action potential,47,48 especially in patients with LQTS.49 IL-6 inhibits cytochrome P450 (CYP450), which increases the bioavailability of QT-prolonging drugs and predisposes to arrhythmias.50 Furthermore, Cytokine storm can cause inflammation in the myocardium. The occurrence of myocarditis following COVID-19 infection has been reported in several studies.50,51 Another proposed mechanism could be the migration of infected alveolar macrophages out of the lung and could potentially increase the risk of arrhythmia by disrupting electrical conduction.44 In addition, it seems that sometimes direct damage to the myocardium as a result of direct involvement of the viral tissue can be a mechanism for the occurrence of myocarditis.52
Figure 2 Effect of the storm of cytokines on the targeted organs and mechanism of arrhythmia on COVID-19.
Another prominent mechanism is the effect of this microbe on the action of angiotensin. The COVID-19 virus uses the spike protein to bind to angiotensin-converting enzyme 2 (ACE2) receptors on the myocardial cell membrane.53 When SARS-CoV-2 binds to ACE2 receptors in the myocardium, the available ACE2 receptors are reduced, causing the accumulation of angiotensin II, leading to adverse myocardial remodeling.54
In the acute phase of myocarditis caused by COVID-19 infection, arrhythmia can occur and the cause can be microvascular disorders caused by hypoxia, gap junctions function disorder due to disorder in the expression of connexin 43, electrolyte imbalance, and also direct cytopathic effects of the virus.45 Also, arrhythmia can occur in the nonacute phase and in the post-inflammatory phase. Some degree of scarring that is created can be the basis for re-entrant tachyarrhythmias.55 Dysfunction of microvascular function and hyper-inflammatory state caused by the activation of inflammatory cells in pre-existing atherosclerotic plaque cause myocardial ischemia. In the event of IHD, the event of inflammation is an essential element in the formation and stability of atherosclerotic plaque. TNF-α facilitates the recruitment and migration of leukocytes through the expression of vascular cell adhesion molecule 1 and causes oxidative stress in atherosclerotic plaques.56,57 IL-1 and IL-6 are chemotactic mediators, and IL-1 levels indicate the presence of unstable atheromatous disease.58
COVID-19 infection sometimes causes systolic heart failure through ischemia or myocarditis. In CHF, the expression of the main proinflammatory cytokines (such as TNF-a, IL-1, and IL-6) by stressed myocytes leads to the creation of an inflammatory environment due to fibroblast recruitment59–61 and macrophages to that place and finally causes chronic myocardial regeneration and fibrosis. Both the inflammatory microenvironment in the acute phase and fibrosis in the chronic phase are susceptible to arrhythmia.44 IL-33, an inflammatory cytokine, plays a pivotal role in the immune response and has a role in pathophysiology of heart failure. ST2 is IL-33 receptor and is involved in cardiac remodeling. Increased ST2 is a predictable biomarker to present the risk factor of heart failure. Higher level of soluble ST2 is associated with increased mortality in individuals with cardiac diseases. Further study of IL-33/ST2 in cardiovascular patients that are involved with COVID-19 is necessary to identify its role in cytokine storm and complicated conditions.62,63
Pulmonary embolism has been reported as the most common thrombotic complication in patients with COVID-19 infection.64–66 Increased pulmonary pressure following pulmonary embolism, ARDS, and heart failure can cause increased pressure on the right atrium, and this stress imposed on the right atrium can be the cause of atrial tachyarrhythmia.67,68 Even transient complete heart block has been seen due to transient increase in pulmonary blood pressure.21
One of the most important complications caused by COVID-19 infection is the occurrence of electrolyte disorders such as hypokalemia, hypomagnesaemia, and hypophosphatemia,69 which can occur due to diarrhea or kidney failure.70 Electrolyte disorders have been reported in 7.2% of patients with COVID-19 infection.17 The relationship between the incidence of arrhythmia and electrolyte disorders has been well recognized.71
Many of the treatments for COVID-19, including azithromycin, hydroxychloroquine, and lopinavir/ritonavir, have a known effect on QT prolongation and the risk of possible TDP.72 Azithromycin and hydroxychloroquine prolong the action potential by inhibiting the hERG-K channel and this, together with unopposed inward Na+ and Ca+2 currents, initiates early depolarization, which can lead to TDP.73 In addition to this fatal side effect of QT prolongation, hydroxychloroquine can also cause advanced AV conduction block.41
Conclusion
The epidemic of COVID-19 infection has been the main health challenge of the last century, which has affected the whole. This disease affects different organs of the body and many side effects have been reported. Among its most serious and deadly complications is the involvement of the cardiovascular system. COVID-19 infection can cause myocardial ischemia, heart failure, myocarditis, and thromboembolic events by stimulating the immune system and creating a cytokine storm that all of these can cause cardiac arrhythmia. Although some cases of arrhythmia are benign, others can be dangerous and even life--threatening. In addition, electrolyte disorders and side effects of COVID-19’s drugs can also trigger the occurrence of fatal arrhythmias. According to several reports, the mortality increases in patients with COVID-19 -infection who are hospitalized in the ICU if arrhythmia occurs and this shows the importance of arrhythmia in the management of these patients. Considering that the COVID-19 infection has affected the whole world, and on the other hand, the occurrence of some arrhythmias is a threat to human life, it is necessary to better understand the pathophysiology and mechanisms involved in the occurrence of arrhythmia caused by corona virus, so that we can do -better to treat them.
Ethics Approval and Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Availability of Data and Materials
Not applicable.
Competing Interest
There is no conflict of interest.
Funding
Not applicable.
Authors’ contributions
CW, EMN, SSA, and WH participated in the design, study, and drafting of the manuscript.
Acknowledgements
Not applicable.
REFERENCES
1. Benjamin EJ, Virani SS, Callaway CW, Chamberlain AM, Chang AR, Cheng S, et al. Heart disease and stroke-statistics-2018 up-date: a report from the American Heart Association. Circulation. 2018;137(12):e67. 10.1161/CIR.0000000000000573
2. Fu D-G. Cardiac arrhythmias: diagnosis, symptoms, and treatments. Cell Biochem Biophys. 2015;73(2):291–296. 10.1007/s12013-015-0626-4
3. Behere SP, Weindling SN. Inherited arrhythmias: the cardiac channelopathies. Ann Pediatr Cardiol. 2015;8(3):210–220. 10.4103/0974-2069.164695
4. Lakkireddy DR, Chung MK, Deering TF, Gopinathannair R, Albert CM, Epstein LM, et al. Guidance for rebooting electrophysiology through the COVID-19 pandemic from the heart rhythm society and the American Heart Association Electrocardiography and Arrhythmias Committee of the Council on Clinical Cardiology. Circ Arrhythm Electrophysiol. 2020;13:e008999. 10.1016/j.hrthm.2020.06.012
5. Jee Y. WHO IHR emergency committee for the COVID-19 outbreak. Epidemiol Health. 2020;42:e2020013. 10.4178/epih.e2020013
6. COVID-19 United States cases by county. Johns Hopkins Coronavirus Resource Center. Available at: https://coronavirus.jhu.edu/us-map. (Accessed May 8, 2020).
7. Kochav SM, Coromilas E, Nalbandian A, et al. Cardiac arrhythmias in COVID-19 infection. Circ Arrhythm Electrophysiol 2020;13:e008719. 10.1161/CIRCEP.120.008719
8. Qu Z, Weiss JN. Mechanisms of ventricular arrhythmias: from molecular fluctuations to electrical turbulence. Ann Rev Physiol. 2015;77:29–55. 10.1146/annurev-physiol-021014-071622
9. Sato D, Xie LH, Sovari AA, Tran DX, Morita N, Xie F, et al. Synchronization of chaotic early afterdepolarizations in the genesis of cardiac arrhythmias. Proc Natl Acad Sci U S A. 2009;106:2983–2988. 10.1073/pnas.0809148106
10. Weiss JN, Garfinke A, Karagueuzian HS, Nguyen TP, Olcese R, Chen P-S, et al. Perspective: a dynamics-based classification of ventricular arrhythmias. J Mol Cell Cardiol. 2015;82:136–152. 10.1016/j.yjmcc.2015.02.017
11. Nasab EM, Athari SS. The first report of 2:1 atrioventricular block following COVID-19 vaccination. Clin Case Rep. 2022;10(5):e05797. 10.1002/ccr3.5797
12. Groleau G, et al. Complete heart block. J Emerg Med. 1986;4(1):25–32. 10.1016/0736-4679(86)90109-5
13. Nasab EM, Heidarzadeh S, Yavari B, Athari SS. Acute upper limb ischemia in a patient with COVID-19: a case report. Ann Vasc Surg. 2021;77:83–88. 10.1016/j.avsg.2021.07.007
14. Lipsitch M, Swerdlow DL, Finelli L. Defining the epidemiology of covid-19 studies needed. N Engl J Med. 2020;382:1194–1196. 10.1056/NEJMp2002125
15. Zhou F, Yu T, Du R, Fan G, Liu Y, Liu Z, et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet. 2020;395:1054–1062. 10.1016/S0140-6736(20)30566-3
16. Rocca DGD, Magnocavallo M, Lavalle C, Romero J, Forleo GB, Tarantino N, et al. Evidence of systemic endothelial injury and microthrombosis in hospitalized COVID-19 patients at different stages of the disease. J Thromb Thrombolysis. 2021;51(3):571–576. 10.1007/s11239-020-02330-1
17. Shi S, Qin M, Shen B, Cai Y, Liu T, Yang F, et al. Association of cardiac injury with mortality in hospitalized patients with COVID-19 in Wuhan, China. JAMA Cardiol. 2020;5:802–810. 10.1001/jamacardio.2020.0950
18. Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. 2020;395(10223):497–506. 10.1016/S0140-6736(20)30183-5
19. Guo T, Fan Y, Chen M, Wu X, Zhang L, He T, et al. Cardiovascular implications of fatal outcomes of patients with coronavirus disease 2019 (COVID-19). JAMA Cardiol. 2020;5(7):811–818. 10.1001/jamacardio.2020.1017
20. Wang D, Hu B, Hu C, et al. Clinical characteristics of 138-hospitalized patients with 2019 novel coronavirus–infected pneumonia in Wuhan, China. JAMA. 2020;323:1061. 10.1001/jama.2020.1585
21. He J, Wu B, Chen Y, Tang J, Liu Q, Zhou S, et al. Characteristic electrocardiographic manifestations in patients with COVID-19. Can J Cardiol. 2020;36(6):966.e1–966.e4. 10.1016/j.cjca.2020.03.028
22. Bhatla A, Mayer MM, Adusumalli S, et al. COVID-19 and cardiac arrhythmias. Heart Rhythm. 2020;17:1439–1444. 10.1016/j.hrthm.2020.06.016
23. Berman JP, Abrams MP, Kushnir A, et al. Cardiac electrophysiology consultative experience at the epicenter of the COVID-19 pandemic in the United States. Indian Pacing Electrophysiol J. 2020;20:250–256. 10.1016/j.ipej.2020.08.006
24. Gopinathannair R, Merchant FM, Lakkireddy DR, Etheridge SP, Feigofsky S, Han JK, et al. COVID-19 and cardiac arrhythmias: a global perspective on ar-rhythmia characteristics and management strategies. J Interv Card Electrophysiol. 2020;59(2):329–336. 10.1007/s10840-020-00789-9
25. Russo V, Rago A, Carbone A, Bottino R, Ammendola E, Della Cioppa N, et al. Atrial fibrillation in COVID-19: from epidemiological association to pharmaco-logical implications. J Cardiovasc Pharmacol. 2020;76(2):138–145. 10.1097/FJC.0000000000000854
26. Chen Q, Xu L, Dai Y, Ling Y, Mao J, Qian J, et al. Cardiovascular manifestations in severe and critical patients with COVID-19. Clin Cardiol. 2020;43(7):796–802. 10.1002/clc.23384
27. Amaratunga EA, Corwin DS, Moran L, Snyder R. Bradycardia in patients with COVID-19: a calm before the storm? Cureus. 2020;12:e8599. 10.7759/cureus.8599
28. Si D, Du B, Ni L, Yang B, Sun H, Jiang N, et al. Death, discharge and ar-rhythmias among patients with COVID-19 and cardiac injury. CMAJ. 2020;192(28):E791–E798. cmaj.200879. 10.1503/cmaj.200879
29. Podrid PJ, Myerburg RJ. Epidemiology and stratification of risk for sudden cardiac death. Clin Cardiol. 2005;28(11 Suppl 1):I3–I11. 10.1002/clc.4960281303
30. Manolis AS, et al. COVID-19 infection and cardiac arrhythmias. Trends Cardiovasc Med. 2020;30:451–460. 10.1016/j.tcm.2020.08.002
31. Singh AP, Tousif S, Umbarkar P, Lal H. A pharmacovigilance study of hydrox-ychloroquine cardiac safety profile: potential implication in COVID-19 mitiga-tion. J Clin Med. 2020;9:E1867. 10.3390/jcm9061867
32. Roden DM, Harrington RA, Poppas A, Russo AM. Considerations for drug inter-actions on QTc interval in exploratory COVID-19 treatment. J Am Coll Cardiol. 2020;75:2623–2624. 10.1016/j.jacc.2020.04.016
33. Yu C-M, Wong RS-M, Wu EB, et al. Cardiovascular complications of severe acute respiratory syndrome. Postgrad Med J. 2006;82:140–144. 10.1136/pgmj.2005.037515
34. Liu K, Fang Y-Y, Deng Y, et al. Clinical characteristics of novel coronavirus cases in tertiary hospitals in Hubei province. Chin Med J (Engl). 2020;133:1025–1031. 10.1097/CM9.0000000000000744
35. Sala S, Peretto G, De Luca G, et al. Low prevalence of arrhythmias in clinically stable COVID-19 patients. Pacing Clin Electrophysiol. 2020;43(8):891–893. 10.1111/pace.13987
36. Saad M, Omrani AS, Baig K, et al. Clinical aspects and outcomes of 70 patients with Middle East respiratory syndrome coronavirus infection: a single-center experience in Saudi Arabia. Int J Infect Dis. 2014;29:301–306. 10.1016/j.ijid.2014.09.003
37. Michael P, et al. Arrhythmias in the COVID-19 patient. Heart Rhythm Soc. 2022;3:8–14. 10.1016/j.hroo.2022.01.002
38. Azarkish M, Laleh Far V, Eslami M, Mollazadeh R. Transient complete heart block in a patient with critical COVID-19. Eur Heart J. 2020;41:2131. 10.1093/eurheartj/ehaa307
39. Kir D, Mohan C, Sancassani R. HEART BRAKEan unusual cardiac manifestation of coronavirus disease 2019 (COVID-19). J Am Coll Cardiol Case Rep. 2020;2:1252–1255.26. 10.1016/j.jaccas.2020.04.026
40. Xiong T-Y, Redwood S, Prendergast B, Chen M. Coronaviruses and the cardiovascular system: acute and long-term implications. Eur Heart J. 2020;4(1):1798–1800. 10.1093/eurheartj/ehaa231
41. Kochi AN, Tagliari AP, Forleo GB, Fassini GM, Tondo C. Cardiac and arrhythmic complications in patients with COVID-19. J Cardiovasc Electrophysiol. 2020;31:1003–1008. 10.1111/jce.14479
42. Babapoor-Farrokhran S, Gill D, Walker J, Rasekhi RT, Bozorgnia B, Amanullah A. Myocardial injury and COVID-19: possible mechanisms. Life Sci. 2020;253:117723. 10.1016/j.lfs.2020.117723
43. Dherange P, Lang J, Qian P, Oberfeld B, Sauer WH, Koplan B, Tedrow U. Arrhythmias and COVID-19: a review. JACC Clin Electrophysiol. 2020;6(9):1193–1204. 10.1016/j.jacep.2020.08.002
44. Lazzerini PE, Boutjdir M, Capecchi PL. COVID-19, arrhythmic risk and inflammation: mind the gap! Circulation. 2020;142: 7–9. 10.1161/CIRCULATIONAHA.120.047293
45. Kolettis TM. Coronary artery disease and ventricular tachyarrhythmia: pathophysiology and treatment. Curr Opin Pharmacol. 2013;13: 210–217. 10.1016/j.coph.2013.01.001
46. Puntmann VO, Taylor PC, Barr A, Schnackenburg B, Jahnke C, Paetsch I. Towards understanding the phenotypes of myocardial involvement in the presence of self-limiting and sustained systemic inflammation: a magnetic resonance imaging study. Rheumatology (Oxford). 2010;4(9):528–535. 10.1093/rheumatology/kep426
47. Lazzerini PE, Laghi-Pasini F, Boutjdir M, Capecchi PL. Cardioimmunology of arrhythmias: the role of autoimmune and inflammatory cardiac channelopathies. Nat Rev Immunol. 2019;19:63–64. 10.1038/s41577-018-0098-z
48. Lazzerini PE, Capecchi PL, Laghi-Pasini F. Long QT syndrome: an emerging role for inflammation and immunity. Front Cardiovasc Med. 2015;2:26. 10.3389/fcvm.2015.00026
49. Lazzerini PE, Capecchi PL, Laghi-Pasini FM. Systemic inflammation and arrhythmic risk: lessons from rheumatoid arthritis. Eur Heart J. 2017;38:1717–1727. 10.1093/eurheartj/ehw208
50. Lazzerini PE, Acampa M, Capecchi PL, et al. Antiarrhythmic potential of anticytokine therapy in rheumatoid arthritis: tocilizumab reduces corrected QT interval by controlling systemic inflammation. Arthritis Care Res. 2015;67:332–339. 10.1002/acr.22455
51. Kobayashi H, Kobayashi Y, Yokoe I, Kitamura N, Nishiwaki A, Takei M, et al. Heart rate-corrected QT interval duration in rheumatoid arthritis and its reduction with treatment with the interleukin 6 inhibitor tocilizumab. J Rheumatol. 2018;45(12):1620–1627. 10.3899/jrheum.180065
52. Lindner D, Fitzek A, Bräuninger H, Aleshcheva G, Edler C, Meissner K, et al. Association of cardiac infection with SARS-CoV-2 in confirmed COVID-19 autopsy cases. JAMA Cardiol. 2020;5(11):1281–1285. 10.1001/jamacardio.2020.3551
53. Wrapp D, Wang N, Corbett KS, et al. Cryo-EM structure of the 2019-nCoV spike in the prefusion conformation. Science. 2020;367:1260–1263. 10.1126/science.abb2507
54. Vaduganathan M, Vardeny O, Michel T, McMurray JJV, Pfeffer MA, Solomon SD. Renin angiotensin–aldosterone system inhibitors in patients with Covid-19. N Engl J Med. 2020;382:1653–1659. 10.1056/NEJMsr2005760
55. Peretto G, Sala S, Rizzo S, et al. Arrhythmias in myocarditis: state of the art. Heart Rhythm. 2019;16:793–801. 10.1016/j.hrthm.2018.11.024
56. Zhang H, Park Y, Wu J, et al., Role of TNF-alpha in vascular dysfunction, Clin Sci (Lond.). 2009;116(3):219–230. 10.1042/CS20080196
57. Zhang G, Cai Q, Zhou H, He C, Chen Y, Zhang P, et al. OxLDL/β2GPI/anti β2GPI Ab complex induces inflammatory activation via the TLR4/NF κB pathway in HUVECs. Mol Med Rep. 2021;23(2):148. 10.3892/mmr.2020.11787
58. Waehre T, Yndestad A, Smith C, et al. Increased expression of interleukin-1 in coronary artery disease with downregulatory effects of HMG-CoA reductase inhibitors. Circulation. 2004;109(16):1966–1972. 10.1161/01.CIR.0000125700.33637.B1
59. Kaptoge S, Seshasai SRK, Gao P, et al. Inflammatory cytokines and risk of coronary heart disease: new prospective study and updated meta-analysis. Eur Heart J. 2014;35(9):578–589. 10.1093/eurheartj/eht367
60. Gullestad L, Ueland T, Vinge LE, Finsen A, Yndestad A, Aukrust P. Inflammatory cytokines in heart failure: mediators and markers. Cardiology. 2012;122(1):23–35. 10.1159/000338166
61. Bozorgi A, Nasab EM. Red cell distribution width and severe left ventricular dysfunction in ischemic heart failure. Crit Pathways Cardiol. 2016;15(4):174–178. 10.1097/HPC.0000000000000094
62. Nasab EM, Makoei RH, Aghajani H, Athari SS. IL-33/ST2 pathway as upper-hand of inflammation in allergic asthma contributes as predictive biomarker in heart failure. ESC Heart Fail. 2022;9(6):3785–3790. 10.1002/ehf2.14111
63. Hami M, Naddaf S, Mobedi I, Zare-Bidaki M, Athari S, Hajimohammadi B, et al. Prevalence of Linguatula serrata infection in domestic bovids slaughtered in Tabriz Abattoir, Iran. Iran J Parasitol. 2009;4(3):25–31.
64. Klok FA, Kruip MJH, van der Meer NJM, et al. Incidence of thrombotic complications in critically ill ICU patients with COVID-19. Thromb Res. 2020;191:145–147. 10.1016/j.thromres.2020.04.013
65. Nasab EM, Heidarzadeh S, Athari SS. Right atrial clot and pulmonary embolism in a patient with COVID-19: a case report. Radiol Case Rep. 2021;16(11):3392–3395. 10.1016/j.radcr.2021.08.015
66. Nasab EM, Athari SS. COVID-19 cytokine storm complications in asthmatic patients. Open Public Health J. 2020;13:625–626. 10.2174/1874944502013010625
67. Wanamaker B, Cascino T, McLaughlin V, Oral H, Latchamsetty R, Siontis KC. Atrial arrhythmias in pulmonary hypertension: pathogenesis, prognosis and management. Arrhythm Electrophysiol Rev. 2018;7:43–48. 10.15420/aer.2018.3.2
68. Ñamendys-Silva SA, Santos-Martínez LE, Pulido T, et al. Pulmonary hypertension due to acute respiratory distress syndrome. Braz J Med Biol Res. 2014;47:904–910. 10.1590/1414-431X20143316
69. Seecheran R, Narayansingh R, Giddings S, et al. Atrial arrhythmias in a patient presenting with coronavirus-disease-2019 (COVID-19) infection. J Investig Med High Impact Case Rep. 2020;8:2324709620925571. 10.1177/2324709620925571
70. Diao B, Wang C, Wang R, Feng Z, Zhang J, Yang H, et al. Human kidney is a target for novel severe acute respiratory syndrome coronavirus 2 infection. Nat Commun. 2021;12(1):2506. 10.1038/s41467-021-22781-1
71. Surawicz B. Role of electrolytes in etiology and management of cardiac arrhythmias. Prog Cardiovasc Dis. 1966;8:364–386. 10.1016/S0033-0620(66)80011-7
72. Giudicessi JR, Noseworthy PA, Friedman PA, Ackerman MJ. Urgent guidance for navigating and circumventing the QTc-prolonging and torsadogenic potential of possible pharmacotherapies for coronavirus disease 19 (COVID-19). Mayo Clin Proc. 2020;95:1213–1221. 10.1016/j.mayocp.2020.03.024
73. Mercuro NJ, Yen CF, Shim DJ, Maher TR, McCoy CM, Zimetbaum PJ, et al. Risk of QT interval prolongation associated with use of hydroxychloroquine with or without concomitant azithromycin among hospitalized patients testing positive for coronavirus disease 2019 (COVID-19). JAMA Cardiol. 2020;5(9):1036–1041. 10.1001/jamacardio.2020.1834
74. Sun Y, Pavey H, Wilkinson I, Fisk M. Role of the IL-33/ST2 axis in cardiovascular disease: a systematic review and meta--analysis. PLoS One. 2021;16(11):e0259026. 10.1371/journal.pone.0259026