
Download
ORIGINAL ARTICLE
Rapid maxillary expansion and nasal patency in mouth breathing children with maxillary atresia due to or not due to allergic rhinitis
Paulo de Tarso Almeida Carvalhoa, Mario Cappellette Juniorb, Gustavo Falbo Wandalsena, Dirceu Soléa*
aDivision of Allergy, Clinical Immunology and Rherumatology – Federal University of São Paulo – Escola Paulista de Medicina (UNIFESP-EPM), São Paulo, Brazil
bDepartment of Otorhinolaryngology, UNIFESP-EPM, São Paulo, Brazil
Abstract
Aim: To evaluate the effects of rapid maxillary expansion (RME) on nasal patency in mouth breathing (MB) children with maxillary atresia due to or not due to allergic rhinitis (AR) associated with asthma.
Methods: Fifty-three MB children/adolescents (aged 7–14 years) with mixed or permanent dentition and maxillary atresia participated, with or without unilateral or bilateral crossbite. They formed the groups: RAD (AR + asthma; clinical treatment, RME); RAC (AR + asthma; clinical treatment, no RME); and D (mouth breathers; RME only). RAD and RAC patients received topical nasal corticosteroid and/or systemic H1 antihistamine (continuous use) and environmental exposure control. All were evaluated before RME (T1) and 6 months after (T2) with the CARATkids score, acoustic rhinometry, and nasal cavity computed tomography (CT). Patients RAD and D underwent RME (Hyrax® orthopedic appliance).
Results: A significant reduction in the CARATkids score occurred in the RAD (−4.06; p < 0.05), similarly when patient and parent/guardian scores were evaluated (−3.28 and −3.16, respectively). Acoustic rhinometry (V5) showed increased nasal volume in all groups, significantly higher in RAD patients than in RAC and D (0.99 × 0.71 × 0.69 cm3, respectively). CT of the nasal cavity documented increased volume in all three groups, with no significant differences between them.
Conclusion: In MB patients with AR, asthma, and maxillary atresia, RME increased nasal cavity volume and improved respiratory symptoms. However, it should not be used as the only treatment for managing patients with respiratory allergies.
Key words: asthma, maxillary atresia, mouth breathing, allergic rhinitis, respiratory system
*Corresponding author: Dirceu Solé, Division of Allergy, Clinical Immunology, and Rheumatology, Rua dos Otonis, 725, Vila Mariana, São Paulo (SP), Brazil. Email addresses: [email protected]; [email protected]
Received 2 February 2023; Accepted 13 April 2023; Available online 1 July 2023
Copyright: Carvalho PDTA, et al.
License: This open access article is licensed under Creative Commons Attribution 4.0 International (CC BY 4.0). http://creativecommons.org/licenses/by/4.0/
Introduction
A mouth breather is any individual who breathes through the mouth due to a pathological adaptation of nasal and/or pharyngeal obstruction.1 In general, the replacement of nasal breathing by mouth breathing (MB) is partial.2,3 There are several causes of MB: choanal atresia, nasal foreign body, nasal septum deformities, nasal masses, and other rare conditions. Among these causes, the most frequent are: hypertrophy of the pharyngeal tonsils (adenoids) and/or palatine tonsils and allergic rhinitis (AR) untreated or uncontrolled.4,5
Nasal breathing in children is essential and is related to the growth of the central facial bones and the functional arrangement of all the muscles involved in breathing and chewing.1,5,6 Chronic nasal obstruction can lead to underdevelopment of the maxillary palatine processes (atresia), resulting in a high-arched hard palate and muscular and postural adaptations to adapt to a new way of breathing, chewing, and even swallowing food.6 Jaw lowering, dental crowding, malocclusion, labial musculature hypotonia, and swallowing changes are observed and may become irreversible if not recognized and treated early. In addition, oral breathing associated with nasal obstruction may predispose to airway collapse and, consequently, sleep respiratory disorders.4,5
In a previous study in which we evaluated patients with MB and dental malocclusion, we documented the presence of rhinitis in 76.4% of patients and confirmed an allergic etiology in 81.7%.5 This is important because AR is often associated with asthma and has been identified as a risk factor for more severe and/or uncontrolled asthma.7–9
The rapid maxillary expansion (RME) is an effective orthopedic procedure that aims to open the palatal suture and determine the appropriate maxillary width. It is indicated for patients with MB, maxillary atresia, and dental malocclusion,10 and can be performed using a variety of fixed and mobile expansion devices.11
RME promotes the separation of the nasomaxillary complex sutures, promoting some skeletal effects, maxillary transversal expansion, which directly affects the piriform aperture, displacement of the nasomaxillary complex downward and forward, increasing the volume of the nasopharynx and oropharynx, which brings respiratory benefits.10 As an orthodontic effect, RME promotes the growth of the maxillary skeleton, better harmonizing the teeth, which become more aligned, improving chewing, swallowing, and speech.10
If the association between MB, dental malocclusion (maxillary atresia), and AR is common, would RME in treating MB affect nasal and/or asthma symptoms in patients with MB and maxillary atresia?
This study aimed to evaluate the effects of RME on nasal patency and control of respiratory disease in children/adolescents with MB and maxillary atresia due to or not due to AR associated with asthma.
Materials and Methods
Sixty-eight children/adolescents (7–14 years old) with mixed or permanent dentition, diagnosed with MB12 and maxillary atresia,13 with or without unilateral or bilateral crossbite,14 were invited to participate. Maxillary atresia is a dentofacial deformity characterized by a discrepancy in the maxilla/mandible relationship in the transverse plane, which may exhibit unilateral or bilateral posterior crossbite.13
All were followed up for at least 6 months at the Allergy Ambulatory Unit of the Department of Allergy, Clinical Immunology and Rheumatology (EPM-UNIFESP) and at the Mouth Breathing Center of the Department of Otorhinolaryngology of the EPM-UNIFESP. Fifteen patients were excluded (eight refused and seven lost the follow-up) and 53 completed the protocol (31 males). These patients were divided into three groups: RAD patients (N = 18), moderate to severe persistent AR (MPAR)9 associated with asthma7 and submitted to RME10; RAC patients (N = 17), MPAR + asthma and without RME; and D patients (N = 18), formed by functional MB patients,12 without AR and asthma, with maxillary atresia and submitted to RME. All children from Groups RAD and RAC had perennial rhinitis and concomitant moderate asthma.
Patient evaluation
On enrolment, all patients underwent clinical assessment, including characterization of allergic sensitivity (at baseline, T1); measurement of nasal cavity permeability by acoustic rhinometry (Rinometrics® rhinometer),15 respiratory symptom score by “CARATkids”16 and computed tomography (CT) of the nasal cavity,17 at baseline (T1) and 6 months later (T2).
Allergic sensitization
All patients were submitted to immediate hypersensitivity skin tests by puncture18 using a standardized battery of inhalant allergens (Dermatophagoides pteronyssinus, Dermatophagoides farinae, Blomia tropicalis, Blatela germanica, Periplaneta americana, fungus mix, dog and cat, IPI-ASAC®), as well as a positive (histamine 1mg/mL) and negative control (saline 0.9%). The test was considered positive if the mean orthogonal diameter of the induced papule was 3 mm greater than the negative control.18 All patients in the RAD and RAC groups showed sensitivity to at least one of the allergens evaluated; those in group D had negative tests.
Symptons score – CARATkids
All patients completed the CARATkids questionnaire, validated for Portuguese (Brazilian culture). The instrument evaluates the presence/interference of rhinitis and asthma symptoms in the child’s/adolescent’s life during the previous 2 weeks. It consists of one part to be answered by the patients (eight questions: three about rhinitis and five about asthma) and another to be answered by the guardians/caregivers (five questions) separately. The sum of the affirmative answers characterizes the CARATkids score (the total varies from 0 to 13; the part for children/-adolescents varies from zero to eight, and that for guardians/-caregivers from zero to five); the higher the score, the worse the control of the respiratory disease.16 Three points from the previous score are the minimum difference capable of detecting worsening or improvement.16 Although the patients of group D did not have AR and/or asthma, they also responded to CARATkids.
Nasal cavity patency
The nasal geometry was assessed by acoustic rhinometry (SER 2000 Rhinometrics® – Denmark), and the volume of the proximal 5 cm of the nasal cavity (V5, cm3) of each nostril was determined, always in triplicate, and after the application of a topical vasoconstrictor (oxymetazoline hydrochloride 0.5 mg/mL). The values were presented as the sum of both nostrils.15,19 The exam was performed with the patient seated after waiting for 20 minutes in an acclimatized environment with a room temperature between 20°C and 22°C and following the standardizations.15
Computed tomography
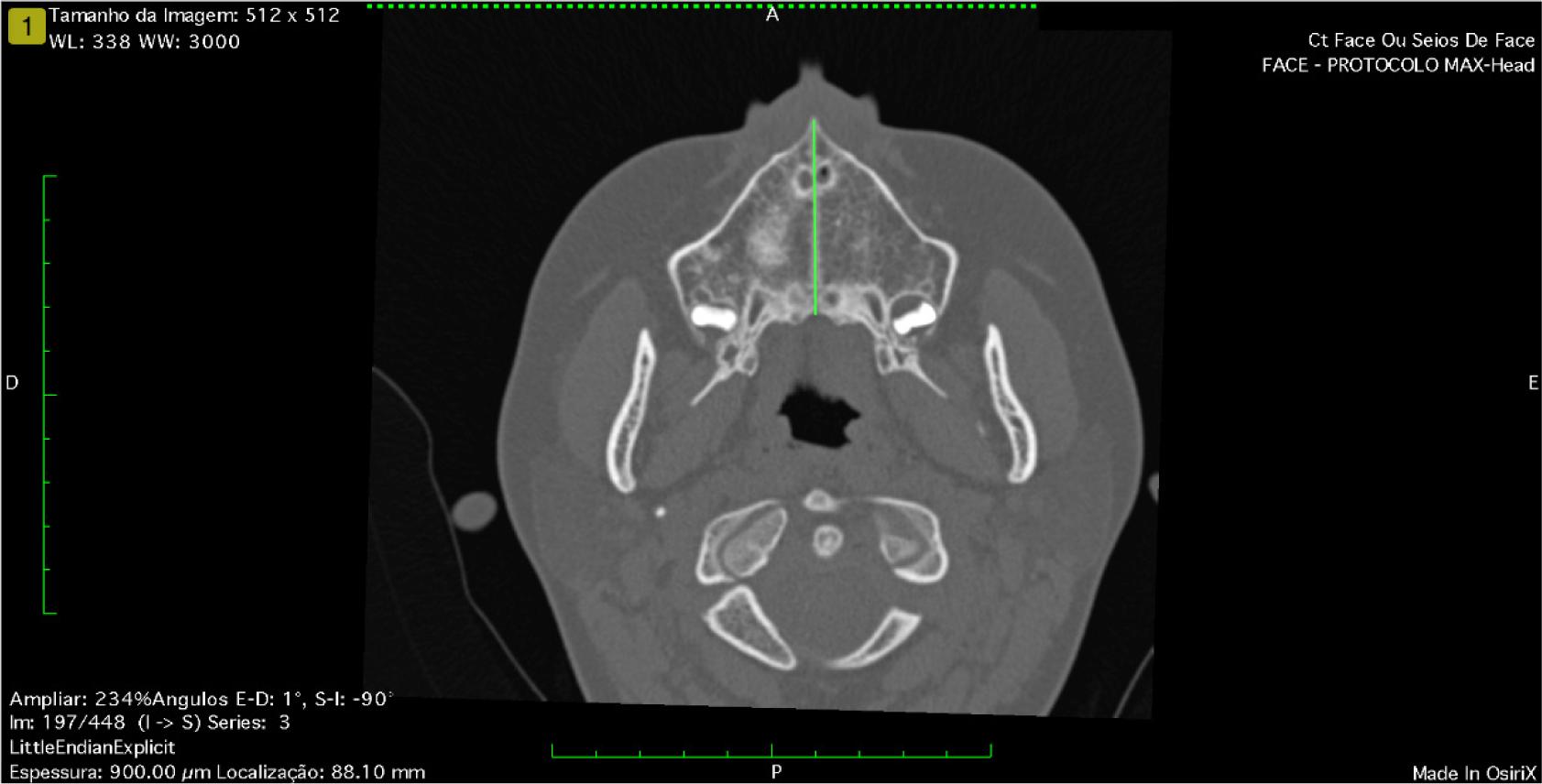
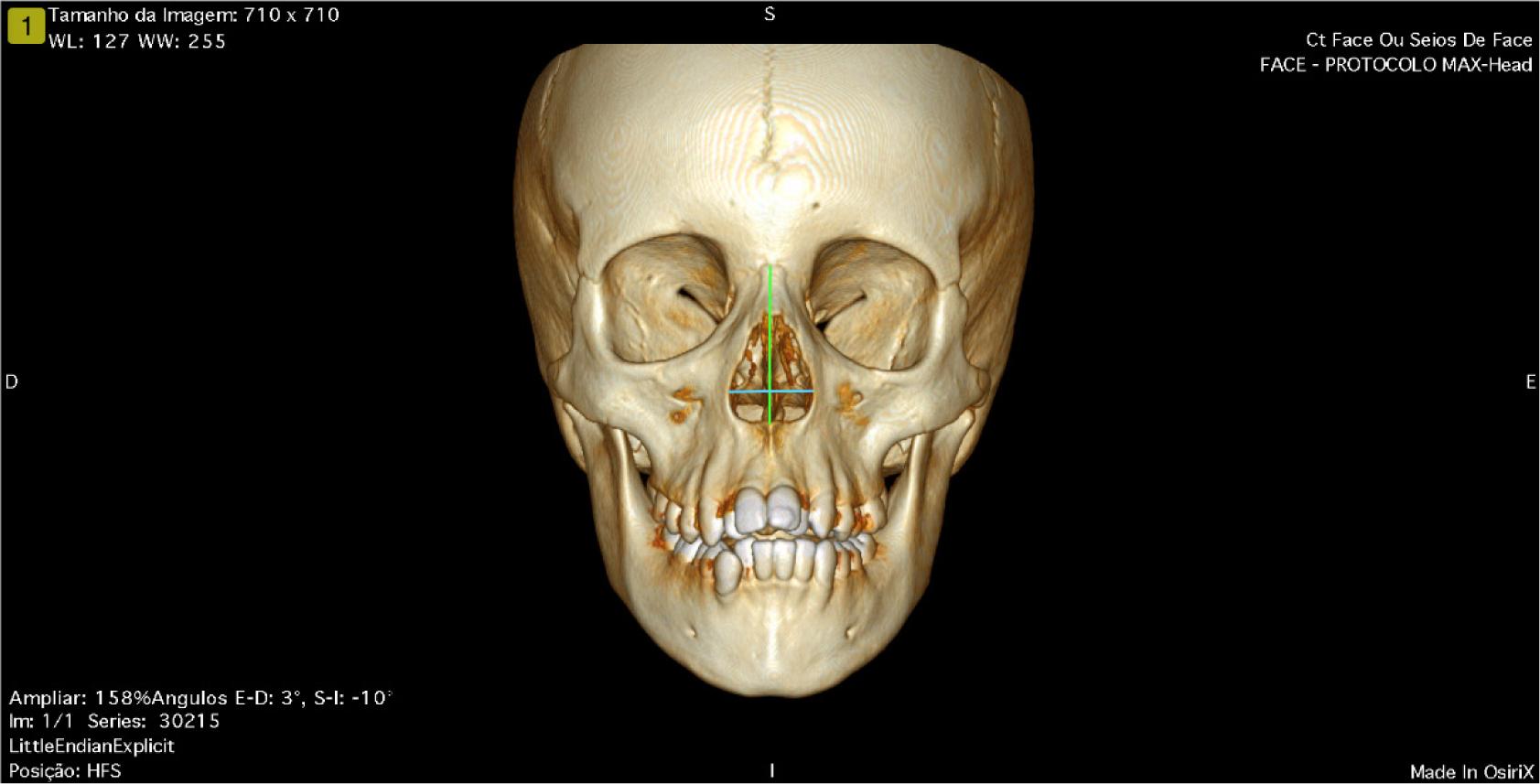
Helical CT was performed at the Department of Diagnostic Imaging (EPM-UNIFESP). The images were exported using specific software to manipulate Digital Imaging and Communication in Medicine (DICOM) images.20 The measurements were performed by the computer program OsiriX Lite (version 9.5.2), which is compatible with DICOM files. A Macbook Pro (Apple®) computer was used, with the following specifications 2.4 GHz Intel® Core I5 processor; 8 GB 1600 MHz DDR3 RAM; 250 GB hard drive. The volume of the nasal cavity was standardized.17 The following linear measurements were obtained: A1: Axial view, the distance between the anterior nasal spine (ANS) and the posterior nasal spine (PNS) (Figure 1); A2: Coronal view, in the 3D reconstructed image, the distance between the ANS and the frontonasal suture (Figure 2); A3: Coronal view, in the 3D reconstructed image, the distance between the most lateral point on the left side and the right side of the pyriform aperture, performed at the first pre-RME scan (Figure 2); and A4: Coronal view, in the 3D reconstructed image, the distance between the most lateral point on the left side and the right side of the pyriform aperture, performed at the second post-RME scan, or 6 months after the first scan.17 The equation obtained the nasal cavity volume at T1: A1 × A2 × A3 = T1 (initial nasal volume), and for the final, A1 × A2 × A4 = T2 (final nasal volume).
Figure 1 Tomographic linear measurement axillary view – A1.
Figure 2 Linear measurement in 3D tomographic image reconstruction – A2 and A3.
The CARATkids score, acoustic rhinometry, and CT were performed at baseline (T1) and 6 months after RME (T2).
Performed treatments
Rapid maxillary expansion
Patients in the RAD and D groups underwent RME with the Hyrax® orthopedic appliance bonded to their teeth (upper molars and premolars) to induce separation of the maxilla in its medial portion, increasing its transverse measurement and consequently, uncrossing the bite, usually achieved within 15 days after appliance activation.21 This moment was defined as T1.
Clinical treatment
Patients in the RAC and RAD groups were treated for AR according to the Allergic Rhinitis and its Impact on Asthma (ARIA) initiative,9,22 with topical nasal corticosteroids and/or systemic H1 antihistamines, both used continuously, in addition to guidance on controlling environmental exposures.23,24 Asthma was treated according to the Global Initiative for Asthma (GINA) guidelines: inhaled corticosteroids at a moderate dose according to age, or a combination of long-acting beta-2 agonists and inhaled corticosteroids twice a day for those older than 4 years, with the quantity adjusted according to age.7
All parents and/or guardians and participating patients were informed about the procedures and signed the Informed Consent and Consent Form. The study was approved by the Research Ethics Committee of UNIFESP-EPM (No. 834.165).
Statistical analysis
Depending on the nature of the variables studied, parametric or nonparametric tests were employed, with a 5% level of rejection of the null hypothesis.
Results
The three study groups were similar in age, and males predominated among the RAD. Namely: RAC: N = 17.53% male, mean age = 10.12 years (standard deviation = 2.78); RAD: N = 18.67% male, mean age = 9.83 years (standard deviation = 2.12); and D: N = 18.56% male, mean age = 10.11 years (standard deviation = 1.45). Patients from RAD and D Groups were submitted to RME and mild local pain was reported by some of them for few hours after the RME. No other side effect was observed.
Table 1 shows the mean results of the evaluated parameters of the patients according to the treatment groups. When analyzing the CARATkids score, we found a significant reduction in the RAD and D groups. Although all groups had similar scores and a decrease in the value, the one that occurred in RAD was significantly higher than the others and bigger than the Decision Making Control Instrument (DMCI) (Table 1, Figure 3).
Table 1 Children and adolescents according to the symptom score obtained by CARATkids total, part related to patients and parents/guardians; the volume of the first 5 cm of the nasal cavity (V5) and volume of the nasal cavity (CT scan) at the beginning (T1), at the end (T2), and the difference between them (T2–T1): with clinical treatment only (RAC), clinical treatment and disjunction (RAD), and disjunction only (D).
| Variable | RAC | RAD | D | ||||||
|---|---|---|---|---|---|---|---|---|---|
| T1 | T2 | T2 – T1 | T1 | T2 | T2 – T1 | T1 | T2 | T2 – T1 | |
| CARATkids score | |||||||||
| Mean | 6.06 | 4.82 | −1.24 | 6.67 | 2.61 | −4.06 | 1.94 | 0.67 | −1.28 |
| Decrease related to all patients* | 8/17 | 17/18 | 15/18 | ||||||
| CARATkids score (children/adolescents) | |||||||||
| Mean | 3.82 | 3.06 | −0.76 | 4.78 | 1.61 | −3.16 | 1.44 | 0.56 | −0.89 |
| Decrease related to all patients* | 8/17 | 17/18 | 12/18 | ||||||
| CARATkids score (parents/guardians) | |||||||||
| Mean | 4.0 | 3.0 | −1.0 | 4.83 | 1.56 | −3.28 | 0.72 | 0.22 | −0.50 |
| Decrease related to all patients* | 8/17 | 15/18 | 9/17 | ||||||
| Acoustic rhinometry V5 (cm3) | |||||||||
| Mean | 7.51 | 8.22 | 0.71 | 7.80 | 8.99 | 0.99 | 8.57 | 9.26 | 0.69 |
| Variation | 4.89–11.46 | 5.82–11.12 | −1.44–2.86 | 5.87–12.81 | 5.01–12.83 | −1.64–3.27 | 5.26–12.55 | 6.12–11.84 | −2.66–3.69 |
| Increase related to all patients* | 12/17 | 13/18 | 12/18 | ||||||
| Computed tomography (cm3) | |||||||||
| Mean | 47.56 | 53.13 | 5.58 | 49.19 | 52.81 | 3.61 | 50.68 | 56.36 | 5.68 |
| Variation | 33.68–71.93 | 31.56–75.05 | 1.08–16.35 | 33.68–65.15 | 36.5–68.37 | −1.06–7.28 | 38.5–63.16 | 43.79–77.45 | 0.89–14.29 |
| Increase related to all patients* | 14/14 | 10/11 | 8/8 | ||||||
*Number of patients who presented the variable according to the total patients evaluated.
CARATKids
Wilcoxon: T1 × T2 – RAC: T1 = T2, p = 0.09; RAD: T1 > T2, p = 0.00015; D: T1 > T2, p = 0.00026.
Kruskal–Wallis: RAC × RAD × D: T1: RAC = RAD > D, p < 0.0001; T2: RAC > RAD > D, p = 0.0001; T2–T1: RAC = D < RAD, p = 0.003.
CARATkids – children/adolescents
Wilcoxon: T1 × T2: RAC: T1 = T2, p = 0.121; RAD: T1 > T2, p = 0.00015; D: T1 > T2; p < 0.001.
Kruskal–Wallis: RAC × RAD × D: T1: RAC = RAD > D, p < 0.0001; T2: RAC > RAD > D, p = 0.001; T2–T1: RAC = D < RAD; p = 0.0020.
CARATkids – parents/guardians
Wilcoxon: T1 × T2: RAC: T2 = T1; p = 0.098; RAD: T2 < T1, p = 0.00035; D: T2 < T1; p = 0.002.
Kruskal–Wallis: RAC × RAD × D: T1: RAC = RAD > D, p = 0.0001; T2: RAC > RAD > D, p = 0.0004; T2–T1: RAD > RAC = D, p = 0.003.
Acoustic rhinometry – V5
Wilcoxon: T1 × T2: RAC: T1 < T2, p = 0.015; RAD: T1 < T2, p = 0.020; D: T1 = T2, p = 0.077.
Kruskal–Wallis: RAD × RAC × D: T1: RAC = RAD = D, p = 0.27; T2: RAC = RAD = D, p = 0.16; T2–T1: RAC = RAD = D, p = 0.93.
Computed tomography – nasal cavity volume
Wilcoxon: T1 × T2: RAC: T2 > T1, p = 0.001; RAD: T2 > T1, p < 0.0001; D: T2 > T1, p = 0.004.
Kruskal–Wallis: RAD × RAC × D: T1: RAC = RAD = D, p = 0.75; T2: RAC = RAD = D, p = 0.89; T2–T1: RAC = RAD = D, p = 0.75.
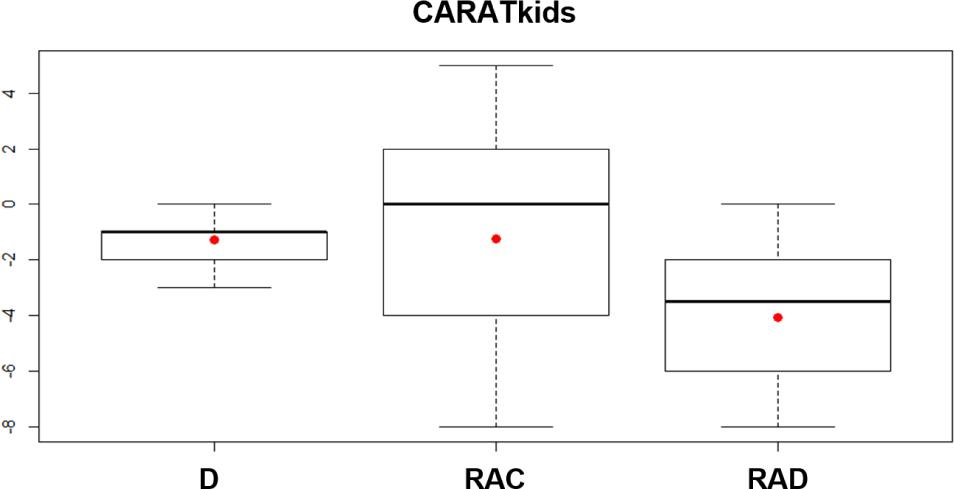
Figure 3 Distribution of the CARATKids score difference (patients and parents/guardians) between the two assessment times according to the study group. D: Disjunction only; RAC: Clinical treatment; and RAD: Clinical treatment and disjunction. Distribution in quartiles. Full horizontal line = median; red dot = mean. Kruskal–Wallis: RAD > D = RAC, p = 0.003.
Individual analysis of the CARATkids components (patient and parent/family scores) showed similar behavior to the combined score: better results for RAD. The same was observed considering the number of patients who showed a favorable change in relation to the total number of patients in the group (Table 1).
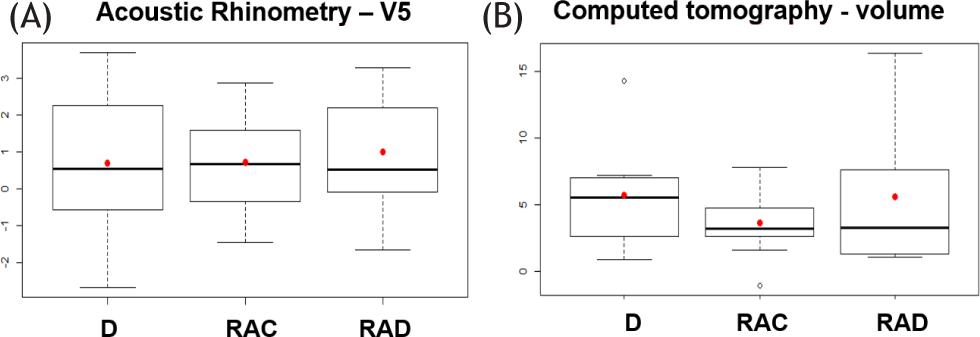
The V5 of the nasal cavity obtained at acoustic rhinometry increased significantly after initiating RAC and RAD treatment. However, there were no significant differences between the three treatment schemes (Table 1, Figure 4).
Figure 4 Distribution of the difference in nasal cavity volume observed by acoustic rhinometry (V5; A) and nasal cavity volume observed by CT scan (B) at the beginning and end according to study group. D: Disjunction only; RAC: Clinical treatment; and RAD: Clinical treatment and disjunction. Distribution by quartiles. Full horizontal line = median; red dot = mean. Kruskal–Wallis – A: D = RAC = RAD; p = 0.93; B: D = RAC = RAD; p = 0.76.
Not all patients had CT nasal cavity volume measurements. The distribution was as follows: RAD (N = 13), RAC (N = 11), and D (N = 11). Statistical analysis showed increased volume after treatment for all three groups and no differences between them (Table 1, Figure 4).
Discussion
In the evaluation of MB patients with maxillary atresia associated or not associated with AR and asthma, we found that the application of RME with a fixed dysfunction appliance improved the scores of respiratory symptoms, in addition to nasal cavity permeability.
The relationship between nasal obstruction and maxillary atresia is clear.5,25 When the patient breathes through the mouth, intraoral pressure increases. Depending on the duration of this habit, the palate shape may change due to the pressure reduction in the nasal cavity, causing maxillary atresia.25,26 The RME, when correcting the maxillary atresia, can cause changes in the nasal cavity, which is confirmed by the improvement of nasal permeability27–30 and the passage of the respiratory flow.31
Some patients evaluated here underwent RME (RAD and D) with the Hyrax® fixed expansion device because it is easy to install, has no acrylic support on the palate, and is easy to clean and adapt. The procedure is somewhat painful. Because it is not removable, it prevents possible patient intervention in the maxillary expansion result.32 According to several authors, the correction of maxillary atresia can be documented about 15 days after its installation. Thus, the natural increase of the airway dimensions becomes irrelevant to the final result.33
To evaluate the role of clinical treatment of AR associated with asthma on nasal cavity permeability, we formed the RAC group, in which there was only continuous clinical treatment for 6 months, as recommended.7,22,24 When comparing the results of the RAD and RAC groups, although the RAC obtained significant increments in the variables studied, those observed in the RAD were higher (Table 1).
We used subjective (CARATkids score)16 and objective (acoustic rhinometry and CT of the face and sinuses) measures15,17 to evaluate nasal permeability and the patient’s response to treatment.
Clinical questionnaires and scores are generally low-cost instruments, mostly easy to understand, quick to apply, and reproducible. The CARATkids, during its validation for the Brazilian culture, was applied to 102 children (6–12 years old) with AR and asthma and compared with other evaluation instruments (asthma and rhinitis) already established.34–38 The results analysis showed that CARATkids has good internal consistency, responsiveness, specificity, and validity in the assessment of asthma and rhinitis.16 It was also possible to classify patients with a score of six or more as having uncontrolled disease, between four and five as having inadequately controlled disease, and score three as having poor control. The minimal clinically significant difference (MCID) in three points was also determined.16 Our study used the CARATKids because it is one of the few instruments validated for use in Brazilian children/adolescents and allows us to evaluate the effect of therapies on AR and asthma together.16
Based on the CARATkids score, RAC and RAD had uncontrolled respiratory disease at the beginning of treatment and changed to insufficiently and poorly controlled respiratory disease, respectively, after treatment. As mentioned above, this assessment was not applied to group D, as they did not have AR and asthma on admission (Table 1). When evaluating the CARATkids scores, improvement was evident in RAD and D, even when patients and parents/guardians were assessed separately. A milder response was expected in the D group since there was no additional antiinflammatory treatment, as they had no respiratory allergy. As part of CARATkids is answered by children, and due to the subjectivity of the symptoms assessment, some influence of these factors may have occurred in the responses of the nonallergic group.
On the other hand, it was clear that in the respiratory allergy groups (RAC and RAD), the improvements were more evident in the RAD group. Although the RAC patients showed a reduction in CARATkids during treatment, this was not significant, perhaps due to the lack of complete control of the inflammatory process underlying AR, as occurred in RAD (Table 1).
For the objective evaluation of nasal patency, we used acoustic rhinometry and CT of the paranasal sinuses, similar to others.39 We submitted patients with AR and normal controls to acoustic rhinometry evaluation in a previous study. We observed a significant negative correlation between nasal resistance, evaluated by active anterior rhinomanometry and acoustic rhinometry parameters. Data analysis revealed that V5 was the parameter with the highest correlation with total nasal resistance, especially in AR patients.40 For this reason, V5 was the parameter chosen for the study of nasal patency because, after this distance, the entry of air into the paranasal sinuses distorts the information obtained,41 and this is the region most affected by RME.42 In all the groups studied here, there was an increase in V5, but without statistical significance.
The evaluation of nasal cavity geometry by acoustic rhinometry has documented results similar to those of CT, mainly when performed in the most anterior region, up to the level of the nasal conchae, precisely the location most affected by RME.43–45 The fact that we could not perform CT in all patients studied compromised the comparison of the two assessments.
While nasal CT showed a volume increase in all three groups, acoustic rhinometry showed a more significant variation in the RAD and RAC groups. This result may have occurred due to the soft tissue influence, as we were able to evaluate the bony portion more accurately with CT. Another factor that may have contributed to this result was the difference in sample size.
The use of acoustic rhinometry and CT of the nasal cavity allowed greater accuracy in evaluating altered structures, as they are not flow dependent, since the nasal area is the same at any respiratory flow. These studies provide us with the exact location of skeletal constrictions and the volume within the nasal cavity.42,46
Conclusion
Considering the results presented here, we conclude that patients with respiratory allergies (AR and asthma) and with maxillary atresia associated with MB show an improvement in the symptoms resulting from the obstructive condition when subjected to RME. However, despite the significant increase in nasal volume and symptom improvement, using RME is not justified solely to control the effects of AR and asthma in allergic patients. However, it is a procedure that can help reduce flares and control respiratory allergies in patients with MB and maxillary atresia.
Statement of ethics
All parents and/or guardians and participating patients were informed about the procedures and signed the Informed Consent and Consent Form. The study was approved by the Research Ethics Committee of UNIFESP-EPM (No. 834.165).
Conflict of interest
The authors declare that there are no potential conflicts of interest regarding this article’s research, authorship, and/or publication
Financial disclosure
The authors declared that no financial support was received for this study.
Authors’ contributions
All the authors contributed equally to the submitted work and approved the final manuscript for its publication.
REFERENCES
1. Di Francesco RC. Respirador oral sem obstáculo das vias aéreas superiores. In: Solé D, Prado E, Weckx LL (eds.), Obstrução nasal – o direito de respirar pelo nariz. 2nd ed. Rio de Janeiro: Atheneu; 2017, p. 69.
2. Garib DG, da Silva Filho OG, Janson G. Etiologia das más oclusões: perspectiva clínica (parte II)–fatores ambientais. Rev Clin Ort Dental Press. 2010;9(3):61–73. Available from: https://br.clinicalorthodontics.net/rcodp-v09n03-2010-61/. Accessed: 21 January 2023.
3. Cappellette M, Jr, Rezende RPDB, Prade KR, Hoppe DPMR, Yamamoto LH, Negrisol S. Controversy: oral or mouth breather, what does the literature say? Ortodontia SPO. 2022;55(4):430–435. Available from: https://fliphtml5.com/wiun/wksj. Accessed: 21 January 2023.
4. Morais-Almeida M, Wandalsen GF, Solé D. Growth and mouth breathers. J Pediatr (Rio J). 2019;95(Suppl. 1):66–71. 10.1016/j.jped.2018.11.005
5. Imbaud TCS, Mallozi MC, Domingos VBTC, Solé D. Frequency of rhinitis and orofacial disorders in patients with dental malocclusion. Rev Paul Pediatr. 2016;34(2):184–8. 10.1016/j.rpped.2015.10.002
6. Valera FC, Anselmo-Lima WT, Tamashiro E. A criança respiradora oral. In: Solé D, Prado E, Weckx LL (Eds.), Obstrução nasal – o direito de respirar pelo nariz. 2nd ed. Rio de Janeiro: Atheneu; 2017, p. 31.
7. Global Initiative for Asthma. Global strategy for asthma management and prevention. 2022. Available from: www.ginasthma.org. Accessed: 22 January 2023.
8. Solé D, Camelo-Nunes IC, Wandalsen GF, Rosario NA, Sarinho EC, Brazilian ISAAC Group. Is allergic rhinitis a trivial disease? Clinics (Sao Paulo). 2011;66(9):1573–1577. 10.1590/s1807-59322011000900012
9. Bousquet J, Anto JM, Bachert C, Baiardini I, Bosnic-Anticevich S, Canonica WG, et al. Allergic rhinitis. Nat Rev Dis Primers. 2020;6(1):95. 10.1038/s41572-020-00227-0
10. Azenha MR, Marzola C, Pereira LC, Pastori CM, Toledo Filho JL. Expansão Rápida da Maxila Cirurgicamente Assistida. Revisão da Literatura, Técnica Cirúrgica e Relato de Caso. Rev Port Estomatol Med Dent Cir Maxil. 2008;49(1):25–30. 10.1016/S1646-2890(08)70031-1
11. Cappellette M, Jr, Fernandes MCPS. Evolução histórica dos aparelhos disjuntores maxilares. In: Cappellette M (Ed.), Disjunção maxilar. 1a ed. Vol. 7. São Paulo: Santos; 2014, pp. 61–63.
12. Menezes VA, Tavares RLO, Granville-Garcia AF. Síndrome da respiração oral: alterações clínicas e comportamentais. Arq Odontol. 2009;45(3):160–165. Available from: https://pesquisa.bvsalud.org/portal/resource/pt/lil-578242.Accessed: 20 January 2023.
13. Rakosi T, Jonas I, Graber TM. Ortodontia e Ortopedia Facial: Diagnóstico. Porto Alegre: Artes Médicas Sul; 1999, pp. 207–209.
14. Silva Filho OG, Silva PRB, Rego MVNN, Capelozza Filho L. Epidemiologia da mordida cruzada posterior na dentadura decídua. J Bras Odontopediatr Odontol Bebê. 2003;6(29): 61–68. Available from: https://pesquisa.bvsalud.org/portal/resource/pt/lil-361663. Accessed: 21 January 2023.
15. Hilberg O, Jackson AC, Swift DL, Pedersen OF. Acoustic rhinometry: evaluation of nasal cavity geometry by acoustic reflection. J Appl Physiol. 1989;66(1):295–303. 10.1152/jappl.1989.66.1.295
16. Amaral R, Carneiro AC, Wandalsen G, Fonseca JA, Solé D. Control of allergic rhinitis and asthma test for children (CARATKids): validation in Brazil and cutoff values. Ann Allergy Asthma Immunol. 2017;118(5):551–556.e2. 10.1016/j.anai.2017.02.007
17. Cappellette M, Jr, Cruz OL, Carlini D, Weckx LL, Pignatari SS. Evaluation of nasal capacity before and after rapid maxillary expansion. Am J Rhinol. 2008;22:74–77. 10.2500/ajr.2008.22.3130
18. Bousquet J, Heinzerling L, Bachert C, Papadopoulos NG, Bousquet PJ, Burney PG, et al. Practical guide to skin prick tests in allergy to aeroallergens. Allergy. 2012;67(1):18–24. 10.1111/j.1398-9995.2011.02728.x
19. Cankurtaran M, Celik H, Coskun M, Hizal E, Cakmak O. Acoustic rhinometry in healthy humans: accuracy of area estimates and ability to quantify certain anatomic structures in the nasal cavity. Ann Otol Laryngol. 2007;116(12):906–916. 10.1177/000348940711601207
20. DICOM – Digital Imaging and Communication in Medicine. Available from: https://www.dicomstandard.org. Accessed: 6 October 2018.
21. Muniz RFL, Gomes RL, Yamamoto LH, Lima LAZ, Cappellette M, Jr. Disjunção da maxila – fase clínica. In: Cappellette M (ed.), Disjunção maxilar. 1a ed. Vol. 9. São Paulo: Santos; 2014, pp. 79–104.
22. Brozek JL, Bousquet J, Agache I, Agarwal A, Bachert C, Bosnic-Anticevich S, et al. Allergic rhinitis and its impact on asthma (ARIA) guidelines–2016 revision. J Allergy Clin Immunol. 2017;140(4):950–958. 10.1016/j.jaci.2017.03.050
23. Rubini N, Wandalsen GF, Rizzo MCV, Aun MV, Chong Neto HJ, Solé D. Guia prático sobre controle ambiental para pacientes com rinite alérgica. Arq Asma Alergia Imunol. 2017;1(1):7–22. 10.5935/2526-5393.20170004
24. Sakano E, Sarinho ESC, Cruz AA, Pastorino AC, Tamashiro E, Kuschnir F, et al. IV Brazilian consensus on rhinitis–an update on allergic rhinitis. Braz J Otorhinolaryngol. 2018;84(1):3–14. 10.1016/j.bjorl.2017.10.006
25. Hitos SF, Solé D, Periotto MC, Fernandes ML, Weckx LL, Guedes ZC. Standardization of the registration and analysis of mastication: proposal for clinical application. Int J Orofacial Myol. 2011;37:47–56. 10.52010/ijom.2011.37.1.4
26. Lione R, Franchi L, Ghislanzoni LTH, Primozic J, Buongiorno M, Cozza P. Palatal surface and volumen in mouth-breathing subjects evaluated with three-dimensional analysis of digital dental casts–a controlled study. Eur J Orthod. 2015;37(1): 101–104. 10.1093/ejo/cju018
27. Agostinho HA, Furtado IA, Silva FS, Ustrell Torrent J. Cephalometric evaluation of children with allergic rhinitis and mouth breathing. Acta Med Port. 2015;28(3):316–321. 10.20344/amp.5556
28. Fastuca R, Campobasso A, Zecca PA, Caprioglio A. 3D facial soft tissue changes after rapid maxillary expansion on primary teeth: a randomized clinical trial. Orthod Craniofac Res. 2018;21(3):140–145. 10.1111/ocr.12229
29. Huang J, Li CY, Jiang JH. Facial soft tissue changes after nonsurgical rapid maxillary expansion: a systematic review and meta-analysis. Head Face Med. 2018;14(1):6. 10.1186/s13005-018-0162-8
30. Radescu OD, Colosi HA, Albu S. Effects of rapid palatal expansion (RPE) and twin block mandibular advancement device (MAD) on pharyngeal structures in Class II pediatric patients from Cluj-Napoca, Romania. Cranio. 2018;23:1–8. 10.1080/08869634.2018.1475940
31. Ottaviano G, Maculan P, Borghetto G, Favero V, Galletti B, Savietto E, et al. Nasal function before and after rapid maxillary expansion in children: a randomized, prospective, controlled study. Int J Pediatr Otorhinolaryngol. 2018;115: 133–138. 10.1016/j.ijporl.2018.09.029
32. Biederman W. A hygienic appliance for rapid expansion. J Pract Orthod. 1968;2(2):67–70.
33. Lotfi V, Ghoneima A, Lagravere M, Kula K, Stewart K. Three-dimensional evaluation of airway volume changes in two expansion activation protocols. Int Orthod. 2018;16(1): 144–157. 10.1016/j.ortho.2018.01.001
34. Ohta K, Bousquet PJ, Akiyama K, Adachi M, Ichinose M, Ebisawa M, et al. Visual analog scale as a predictor of GINA-defined asthma control: the SACRA study in Japan. J Asthma. 2013;50:514–521. 10.3109/02770903.2013.786726
35. Bousquet PJ, Combescure C, Neukirch F, Klossek JM, Méchin H, Daures J-P, et al. Visual analog scales can assess the severity of rhinitis graded according to ARIA guidelines. Allergy Eur J Allergy Clin Immunol. 2007;62:367–372. 10.1111/j.1398-9995.2006.01276.x
36. Spector SL, Nicklas RA, Chapman JA, Bernstein IL, Berger WE, Blessing-Moore J, et al. Symptom severity assessment of allergic rhinitis: part 1. Ann Allergy Asthma Immunol. 2003;91:105–114. 10.1016/s1081-1206(10)62160-6
37. Meltzer EO, Schatz M, Nathan R, Garris C, Stanford RH, Kosinski M. Reliability, validity, and responsiveness of the rhinitis control assessment test in patients with rhinitis. J Allergy Clin Immunol. 2013;131:379–386. 10.1016/j.jaci.2012.10.022
38. Liu AH, Zeiger R, Sorkness C, Mahr T, Ostrom N, Burgess S, et al. Development and cross-sectional validation of the childhood asthma control test. J Allergy Clin Immunol. 2007;119:817–825. 10.1016/j.jaci.2006.12.662
39. Ottaviano G, Fokkens WJ. Measurements of nasal airflow and patency: a critical review with emphasis on the use of peak nasal inspiratory flow in daily practice. Allergy. 2016;71(2):162–174. 10.1111/all.12778
40. Wandalsen GF, Mendes AI, Solé D. Correlation between nasal resistance and different acoustic rhinometry parameters in children and adolescents with and without allergic rhinitis. Braz J Otorhinolaryngol. 2012;78(6):81–86. 10.5935/1808-8694.20120038
41. Nathan RA, Sorkness CA, Kosinski M, Schatz M, Li JT, Marcus P, et al. Development of the asthma control test: a survey for assessing asthma control. J Allergy Clin Immunol. 2004;113(1):59–65. 10.1016/j.jaci.2003.09.008
42. Vidotti BA, Trindade IEK. The effects of rapid maxillary expansion on the nasal patency assessed by rhinomanometry and acoustic rhinometry. R Dental Press Ortodon Ortop Facial. 2008;13(5):59–65. 10.1590/S1415-54192008000600008
43. Doruk C, Sökücü O, Biçakçi AA, Yilmaz U, Tas F. Comparison of nasal volume changes during rapid maxillary expansion using acoustic rhinometry and computed tomography. Eur J Orthod. 2007;29(3):251–255. 10.1093/ejo/cjl069
44. Muñoz-Cano R, Salvador R, Valero A, Berenguer J, Alobid I, Bartra J, et al. Accuracy of acoustic rhinometry versus computed tomography in the evaluation of nasal cavity in patients with nasal polyposis. Rhinology. 2010;48(2):224–227. 10.4193/Rhin09.067
45. Tsolakis IA, Venkat D, Hans MG, Alonso A, Palomo JM. When static meets dynamic: comparing cone-beam computed tomography and acoustic reflection for upper airway analysis. Am J Orthod Dentofacial Orthop. 2016;150(4):643–650. 10.1016/j.ajodo.2016.03.024
46. Zancanella E, Lima WTA. Acousticrhinometry as a diagnosticmethod. Rev Bras Otorrinolaringol. 2004;70(4):500–503. 10.1590/S0034-72992004000400010