
Download
RESEARCH ARTICLE
Factors associated with allergic rhinitis and combined allergic rhinitis and asthma syndrome (CARAS) in adults undergoing immunotherapy in a tropical country: Is ISAAC-III questionnaire useful in adult populations?
Augusto Peñarandaa,b,c, Lucía C. Pérez-Herreraa,b, Manuela Gantivaa,b,d, Sergio Moreno-Lópeza,b, Julian Manriquea,e, Daniel Peñarandac,d, Elizabeth Garcíaa,b,d*
aSchool of Medicine, Universidad de Los Andes, Bogotá, Colombia
bDepartmen of Otolaryngology, Fundación Santa Fe de Bogotá, Bogotá, Colombia
cAllergy and Otolaryngology Research Groups, UNIMEQ-ORL, Bogotá, Colombia
dSection of Otolaryngology, Fundación Universitaria de Ciencias de la Salud – Hospital de San José, Bogotá, Colombia
eAllergy section, Department of Pediatrics, Fundación Santa Fe de Bogotá, Bogotá, Colombia
Abstract
Background: Allergic diseases affect about 10–30% of the population in low- or middle-income tropical countries. Few studies describe the factors associated with allergic diseases in adult patients undergoing immunotherapy in Latin American countries.
Objective: This study aimed to determine the factors associated with allergic rhinitis (AR) and AR in comorbidity with asthma (CARAS) in adults treated with immunotherapy in two allergy referral centers in Bogotá (Colombia).
Material and Methods: Observational, cross-sectional study conducted between January 2018 and January 2019. ISAAC-III and sociodemographic questionnaires were applied to determine the factors associated with AR and CARAS in adults treated with immunotherapy who attended the allergy consult at the Fundación Santa Fe de Bogotá and Unimeq-Orl.
Results: Among 416 adults aged 18–68 years, 71.4% (n = 297) were women. Regarding the sensitization results obtained by skin prick test, the most frequent allergens were house dust mites (64.18%): 49.03% were positive for both Dermatophagoides pteronyssinus and Dermatophagoides farinae, while 28.61% were positive for Blomia tropicalis. Excluding house dust mites, the most frequent allergens were dog hair (31.01%), cat hair (15.1%), grasses (15.9%), and food (15.9%). The main factor associated with exclusive AR was regular acetaminophen use more than four times a year: Prevalence ratio (PR) = 1.77 (95% CI: 1.12–2.25). The main factor associated with CARAS was cesarean delivery PR: 1.44 (95% CI: 1.09–1.78).
Conclusion: The main factor associated with AR was regular acetaminophen use, while that associated with CARAS was cesarean delivery. The ISAAC-III questionnaire can be a useful low-cost tool to assess the factors associated with allergic diseases in adults in tropical countries.
Key words: Allergy, Allergic Rhinitis, Adult Asthma, Atopic Dermatitis, Allergen Immunotherapy, Tropical Climate
*Corresponding author: Elizabeth García, Fundación Santa Fe de Bogotá, Avenida 9 No. 116-20, Office 211, Bogotá 110111, Colombia. Email address: [email protected]
Received 6 February 2023; Accepted 30 March 2023; Available online 1 July 2023
Copyright: Peñaranda A, et al.
License: This open access article is licensed under Creative Commons Attribution 4.0 International (CC BY 4.0). http://creativecommons.org/licenses/by/4.0/
Introduction
The epidemiology of allergic diseases may be particularly different in tropical countries compared to high--income tempered countries.1,2 In sensitized patients, an environmental antigen (allergen) triggers immunoglobulin E–mediated inflammatory reactions.2 These environmental allergens may fluctuate among different geographic and socioeconomic conditions that prompt the existence of specific allergens.2–4 Current studies suggest that environmental variations induced by industrialization and climate change could partially explain the increase in the prevalence and severity of allergic disease, particularly in tropical countries.4 Overall, a high prevalence of allergic diseases has been described in tropical countries due to geographical and environmental characteristics.1,4 Allergic rhinitis (AR), asthma, and atopic dermatitis (AD) are the most frequent chronic diseases in childhood, with a worldwide prevalence of 33, 14, and 24%, respectively.5–7 Several epidemiologic studies assessing the prevalence and factors associated with allergic diseases have been performed worldwide such as the International Study of Asthma and Allergies in Childhood phase III (ISAAC-III).8,9 The ISAAC-III provides standardized data collection strategies for the epidemiologic research of allergic diseases.9
Despite ISAAC-III being initially developed for pediatric populations, a current study applied this self-reported tool together with an objective measure to assess the epidemiology of allergic diseases in an adult population.10 As self--reported suspicion is not enough for the diagnosis of allergic diseases, objective measures such as specific allergen tests (i.e., skin prick test [SPT]) should be performed.11–13 The SPT is a low-cost and minimally invasive sensitization test with a high positive predictive value (95–100%) for the diagnosis of IgE-mediated allergic diseases.13,14 Moreover, SPT allows the identification of specific allergens that are related to allergic symptoms. The most frequent allergens in tropical countries are house dust mites (Blomia tropicalis, Dermatophagoides pteronyssinus and Dermatophagoides farinae), animal hair (dog, cat, horse, and others), and pollen (cypress, ash, etc).1,15 Targeting these allergens that trigger with immunotherapy has proved effective in the control of allergy symptoms, improvement of quality of life, increasing tolerance to allergen exposure, and leading to a reduction in conventional pharmacological treatment.16 Immunotherapy involves the frequent administration of high doses of standardized extracts of allergens via subcutaneous or sublingual route.16–18
Colombia is one of the tropical Latin American countries with the highest prevalence of allergic diseases.3,19 However, research on the epidemiology, medical, and sociodemographic factors associated with allergic diseases in adults using standardized methods is scarce.3,20 To date, no studies in Latin America assessed the factors associated with allergic diseases confirmed by SPT in patients undergoing specific immunotherapy. This study aimed to describe the medical, sociodemographic, and environmental factors associated with AR and asthma syndrome (CARAS)21 in adults aged 18–68 years undergoing specific immunotherapy in two allergy referral centers in Bogotá, Colombia: Fundación Santa Fe de Bogotá (FSFB) and Unidad-Medicoquirúrgica del ORL (UNIMEQ-ORL).
Materials and Methods
Study design
This is an observational, cross-sectional study conducted between January 2019 and January 2020 at the FSFB and UNIMEQ-ORL. The factors associated with AR and CARAS were determined by applying the self-administered ISAAC-III questionnaire in adult patients. All patients had a clinical diagnosis of AR or CARAS, confirmed with SPT, and were undergoing specific immunotherapy. The diagnosis of AR and CARAS and the prescription of immunotherapy were performed by allergists based on the European Academy of Allergy and Clinical Immunology (EAACI) guidelines16,22 and who were trained to support the fieldwork of this research. A sociodemographic questionnaire was also applied.
The FSFB and UNIMEQ-ORL are located in the capital city, and both institutions are allergy and immunotherapy referral centers that treat the population of all socioeconomic statuses. For this study, socioeconomic statuses were classified based on the strata classification of the Colombian National Administrative Department of Statistics (DANE) as follows: low-income (strata I and II), middle--income (strata III and IV), and high-income levels (strata V and VI). DANE uses income data, property information, and people’s households’ residential characteristics to determine this stratification.23 The study was approved by the Ethics Committee of the Hospital Universitario Fundación Santa Fe de Bogotá (CCEI-10248-2019) according to the Helsinki Declaration. All patients included in this study signed informed consent for participation, and no incentives were offered for study participation.
Study population
The study population should meet the following inclusion criteria according to the EAACI guidelines16: (a) Patients aged 18–68 years; (b) Positive SPT results (IgE sensitization) to one or more clinically relevant allergens; (c) Moderate to severe symptoms of the allergic disease that affected their daily activities or sleep and remained despite pharmacotherapy and/or allergen avoidance strategies; (d) Undergoing immunotherapy between 2019 and 2020.
ISAAC-III Questionnaire
The ISAAC-III questionnaire was applied to patients who met the inclusion criteria during the immunotherapy appointments. This questionnaire aims to determine the frequency trends and factors associated with allergic diseases and was priorly adapted and validated in Spanish language.24 The ISAAC-III questionnaire is a low-cost tool to evaluate the frequency of AR, asthma, and AD, as well as their associated factors, with adequate reproducibility and validity.8,9,25 Following the ISAAC-III guidelines’ recommendations, the prevalence of allergic diseases was defined as follows:
-
AR symptoms: A positive response to the ISAAC-III question: “In the last 12 months, have you had a problem with sneezing, snoring, or mouth blockage when you did not have a cold/flu?”.
-
Asthma symptoms: “A positive response to: Have you ever had wheezing or whistling in the chest in the last 12 months?”.
-
AD symptoms: “Have you ever had an itching or rash that came and went for at least 6 months or at any time in the last 12 months?”.
ISAAC-III questionnaire also assesses the factors associated with allergic diseases in pediatric populations (i.e., acetaminophen use, fast food consumption, exercise, smoking exposure, pet-owning).24,26 We applied this Spanish version of the ISAAC-III questionnaire as all these questions were validated prior.24
Statistical analysis
The statistical analysis was performed using Stata16MP. The significance level for the comparisons was priorly established as 5%. In the descriptive analysis, absolute and relative frequencies were calculated for the qualitative variables. Conversely, for the quantitative variables, central tendency measures (average and median) were estimated. For the dispersion measures, standard deviation and interquartile range were calculated along with maximum and minimum values. Height and weight were extracted from the clinical database of the FSFB. The body mass index (BMI) was adjusted by age group and sex according to World Health Organization standards.27 A multivariate analysis based on a logistic regression model was made to identify the variables associated with AR and CARAS. These variables were included in the model considering biological plausibility and statistical associations with a P < 0.2. Odds ratio was converted into prevalence ratio (PR).28,29 Finally, the diagnosis of the models was performed using linearity and goodness-of-fit tests, assessment of collinearity, evaluation of deviance residuals, and leverage points.
Results
A total of 416 adults aged 18–68 years were included, of which 71.4% were females. Overall, 65.1% of the population belonged to a middle-income socioeconomic status, and 31.5% of the total population was overweight or obese. Up to 32.7% of the population remained in immunotherapy treatment for at least 6–12 months. The baseline demographic characteristics of the study population are described in Table 1.
Table 1 Baseline demographic and clinical characteristics of the study population.
| Variables | n = 416 | |
|---|---|---|
| n | % | |
| Sex, Female/Male | 297/119 | 71.4/28.6 |
| Age in years* | 33.8 (12.4) | 31.6 (22.7–42.3) |
| Age group | ||
| 18–40 years old | 296 | 71.2 |
| 41–60 years old | 104 | 25.0 |
| More than 60 years old | 16 | 3.8 |
| Socioeconomic status | ||
| Low-income levels | 123 | 29.6 |
| Middle-income levels | 271 | 65.1 |
| High-income levels | 22 | 5.3 |
| Educational level | ||
| None | 7 | 1.7 |
| Primary education | 23 | 5.5 |
| Secondary education | 101 | 24.3 |
| Technical degree | 67 | 16.1 |
| Higher degree/Education | 171 | 41.1 |
| Other | 46 | 11.1 |
| No data | 1 | 0.2 |
| Mother’s educational level | ||
| None | 9 | 2.2 |
| Primary education | 107 | 25.7 |
| Secondary education | 115 | 27.6 |
| Technical education | 80 | 19.2 |
| Higher education | 79 | 19.0 |
| Other | 21 | 5.0 |
| No data | 5 | 1.2 |
| Father’s educational level | ||
| None | 11 | 2.6 |
| Primary education | 107 | 25.7 |
| Secondary education | 97 | 23.3 |
| Technical education | 69 | 16.6 |
| Higher education | 97 | 23.3 |
| Other | 21 | 5.0 |
| No data | 14 | 3.4 |
| Weight in kg* | 38.6 (11)* | 62 (55–70)* |
| Height in cm* | 163 (8.9)* | 163 (140–169.5)* |
| BMI** | 23.8 (1.3) | 23.5 (21.5–25.9) |
| BMI score classification** | ||
| Underweight | 23 | 5.5 |
| Normal weight | 262 | 63.0 |
| Overweight | 104 | 25.0 |
| Obesity | 27 | 6.5 |
| Exercise frequency per week | ||
| Occasionally or none | 167 | 40.1 |
| 1 to 2 times per week | 135 | 32.5 |
| 3 or more times per week | 113 | 27.2 |
| No data | 1 | 0.2 |
| Smoking | 18 | 4.3 |
| Parents or siblings with | ||
| Allergic rhinitis | 238 | 57.2 |
| Atopic dermatitis | 138 | 33.2 |
| Current exposure to pets | ||
| Dog | 129 | 31.0 |
| Cat | 63 | 15.1 |
| Frequency of acetaminophen use during the last year | ||
| Never | 30 | 7.2 |
| Less than 4 times per year | 156 | 37.5 |
| More than 4 times per year | 230 | 55.3 |
| Length of immunotherapy | ||
| Less than 6 months | 138 | 33.2 |
| 6–18 months | 136 | 32.7 |
| 18–36 months | 115 | 27.6 |
| 36–48 months | 13 | 3.1 |
| More than 48 months | 14 | 3.4 |
*Values are expressed in Mean (SD) and Median (p25–p75)
**WHO categories (BMI: Body Mass Index)
About the SPT sensitization results, the most frequent allergens were house dust mites (64.18%): 49.03% were positive for both D. pteronyssinus and D. farinae, and 28.61% for B. tropicalis. Excluding house dust mites, the most frequent allergens were dog hair (31.01%), cat hair (15.1%), grasses (15.9%), and food (15.9%).
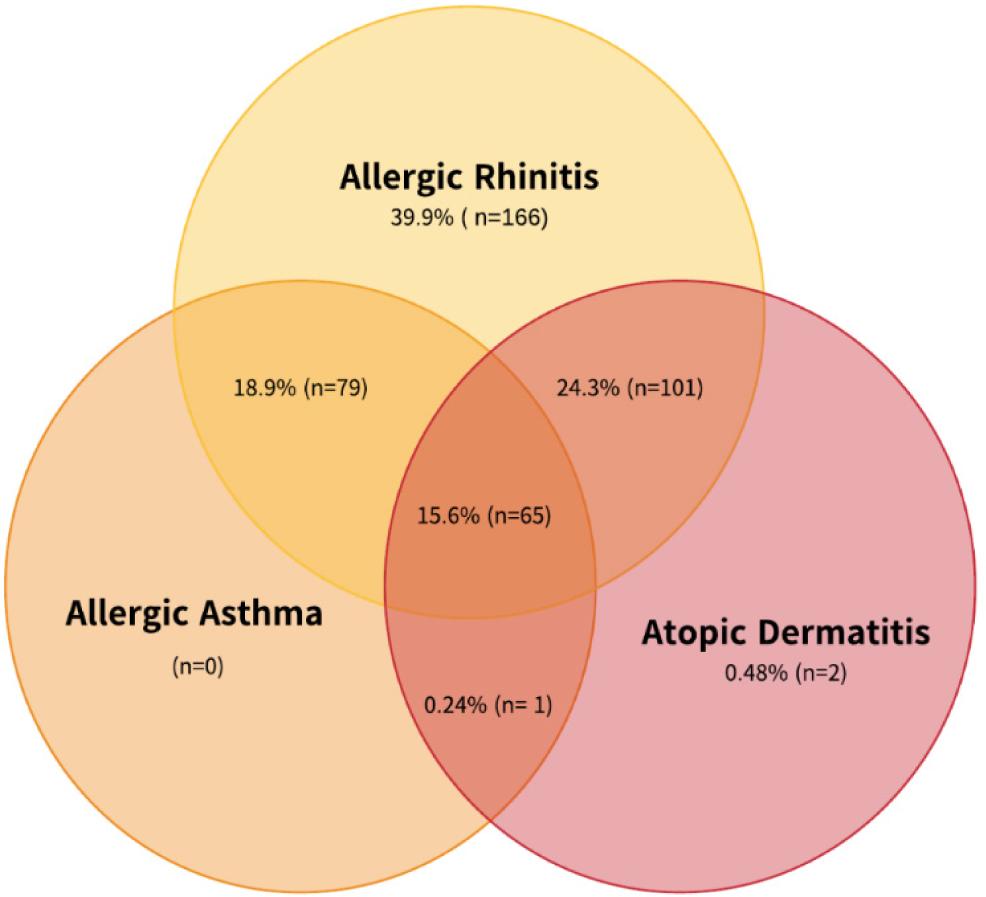
Frequency of allergic diseases
Overall, 39.9% of the population presented with exclusive AR. AR was frequently found in comorbidity with asthma (CARAS: 18.9%) and AD (24.3%). The combination of the three allergic diseases was found in 15.63% of the population. These results are shown in Figure 1 and Table 2.
Figure 1 Frequency of allergic diseases in the study population.
Table 2 Frequency of allergic diseases in the study population.
| Allergic disease | n = 416 | ||
|---|---|---|---|
| n | % | CI 95% | |
| Exclusive allergic rhinitis | 166 | 39.9 | (35.3–44.7) |
| Exclusive asthma | 0 | 0 | - |
| Exclusive atopic dermatitis | 2 | 0.48 | (0.13–1.74) |
| Allergic rhinitis in combination with: | |||
| Asthma | 79 | 18.9 | (15.5–23.3) |
| Atopic dermatitis | 101 | 24.3 | (20.4–28.6) |
| Asthma in combination with Atopic dermatitis | 1 | 0.24 | (0.05–1.3) |
| Presence of allergic rhinitis, asthma, and atopic dermatitis | 65 | 15.63 | (12.4–19.4) |
Factors associated with exclusive AR and CARAS
The factors associated with AR and CARAS were based on a logistic regression model. The PR and 95% confidence intervals for each association are described in Table 3 and Table 4 for for AR and CARAS, respectively. The main factor associated with exclusive AR was regular acetaminophen use more than four times a year PR:1.77 (95% IC: 1.12–2.25). Meanwhile, the main factor associated with AR in comorbidity with asthma (CARAS) was cesarean delivery PR: 1.44 (95% CI: 1.09–1.48).
Table 3 Logistic regression model of the factors associated with allergic rhinitis.
| Variable* | Bivariate analysis | Multivariate analysis | ||
|---|---|---|---|---|
| PR** | 95% IC | PR** | 95% CI | |
| Age in years | 0.99 | (0.98–1.00) | 0.99 | (0.98–1.00) |
| Sex | ||||
| Male | 1.31 | (1.01–1.60) | 1.18 | (0.88–1.50) |
| Socioeconomic status | ||||
| Middle-income levels | 1.14 | (0.86–1.44) | 1.13 | (0.83–1.46) |
| High-income levels | 0.99 | (0.50–1.63) | 0.92 | (0.41–1.62) |
| Cesarean delivery | 1.06 | (0.78–1.36) | 0.98 | (0.69–1.31) |
| Mother’s educational level | ||||
| Secondary education | 1.10 | (0.79–1.42) | 0.84 | (0.54–1.22) |
| Higher education | 1.13 | (0.85–1.43) | 0.86 | (0.55–1.24) |
| Frequency of acetaminophen use | ||||
| Less than 4 times a year | 1.62 | (0.98–2.16) | 1.62 | (0.99–2.15) |
| More than 4 times a year | 1.83 | (1.19–2.31) | 1.77 | (1.12–2.25) |
| Dog ownership at home | 1.07 | (0.82–1.34) | 1.01 | (0.74–1.31) |
| Cat ownership at home | 1.04 | (0.73–1.38) | 1.00 | (0.66–1.38) |
| Fast food consumption | ||||
| 1–2 times per week | 1.21 | (0.93–1.50) | 1.09 | (0.79–1.43) |
| 3 or more times per week | 0.75 | (0.28–1.48) | 0.47 | −1.21) |
Bold numbers highlight the significant associated factors with adequate 95% confidence intervals.
*Log-likelihood (only intercept): −262.644; Log-likelihood of the model: −254.741; AIC: 537.482; BIC: 593.079
**PR: Prevalence ratios
Table 4 Logistic regression model of the factors associated with CARAS.
| Variable(a) | Bivariate analysis | Multivariate analysis | ||
|---|---|---|---|---|
| PR** | 95% IC | PR** | 95% CI | |
| Age in years | 1.00 | (0.99–1.01) | 1.01 | (0.99–1.02) |
| Sex | ||||
| Male | 0.74 | (0.52–1.01) | 0.86 | (0.59–1.18) |
| Socioeconomic status | ||||
| Middle-income levels | 0.87 | (0.63–1.14) | 0.90 | (0.63–1.22) |
| High-income levels | 1.21 | (0.67–1.77) | 1.31 | (0.67–1.97) |
| Cesarean delivery | 1.38 | (1.03–1.74) | 1.44 | (1.09–1.78) |
| Mother’s educational level | ||||
| Secondary education | ||||
| Higher education | 0.96 | (0.65–1.33) | 1.08 | (0.72–1.49) |
| Frequency of acetaminophen use | 0.89 | (0.61–1.21) | 1.00 | (0.64–1.40) |
| Less than 4 times a year | 0.53 | (0.27–0.94) | 0.60 | (0.29–1.08) |
| More than 4 times a year | 0.81 | (0.46–1.27) | 0.86 | (0.46–1.39) |
| Dog ownership at home | 0.98 | (0.72–1.28) | 1.10 | (0.81–1.42) |
| Cat ownership at home | 0.80 | (0.51–1.17) | 0.84 | (0.53–1.23) |
| Fast food consumption | ||||
| 1–2 times per week | 0.81 | (0.56–1.10) | 0.86 | (0.57–1.20) |
| 3 or more times per week | 1.18 | (0.57–1.89) | 1.43 | (0.70–2.12) |
| Overweight or obesity | 1.19 | (0.89–1.51) | 1.07 | (0.78–1.39) |
Bold numbers highlight the significant associated factors with adequate 95% confidence intervals.
*Log-likelihood (only intercept): −253.048; Log-likelihood of the model: −243.191; AIC: 516.381; BIC: 575.950
**PR: Prevalence Ratios
Regarding the diagnosis of these regression models, linearity tests and goodness-of-fit tests were carried out and no collinearity problems were found. During the evaluation of deviance residuals and leverage points, no extreme or influential values that could affect the model were found.
Discussion
This study aimed to describe the medical, sociodemographic, and environmental factors associated with AR and CARAS in adults between 18 and 68 years treated with specific immunotherapy in two reference allergy centers from a tropical country. All the patients included in this study were undergoing specific immunotherapy according to EAACI guidelines,16 and up to 32.7% of them remained in immunotherapy for at least 6–12 months. Therefore, all of the population had a diagnosis of moderate to severe AR symptoms confirmed through clinical diagnosis and an allergy sensitization assessment. Therefore, our results should be interpreted considering this limitation as the population with mild symptoms of AR may have different associated factors. Few studies have been conducted on the epidemiology of allergic diseases in Latin American populations, and most of these studies mostly focused on pediatric populations.30,31 Further studies in diverse Latin American populations are needed to understand the role of different geographic and environmental characteristics that prompt allergens and allergic diseases.
ISAAC-III questionnaires were initially developed for pediatric populations, and few studies have applied this questionnaire to adult populations, which may be considered a limitation of this study. However, ISAAC-III is a low-cost, internationally standardized tool, and prior studies suggest a high correlation between this tool and the ECRHS (European Community Respiratory Health Survey), which is a European questionnaire to assess respiratory allergies in adult populations.32 However, ECRHS does not assess the presence of AD, which is an important factor priorly associated with respiratory diseases.32 Moreover, the ISAAC strategy granted the improvement and modification of the ISAAC questionnaires including wider evidence about the main factors associated with allergic diseases. Several studies support ISAAC-III’s effectiveness and reliability to assess factors associated with allergic disease.9,24,25,32 In low- or middle-income countries, there is limited scientific information about the epidemiology of allergic diseases using standardized methodologies, probably due to budget limitations in scientific research.33–35 Therefore, in these Latin American countries, the ISAAC-III tool may be particularly useful to assess the prevalence trends and factors associated with these diseases.
In Colombia, the national prevalence of self-reported allergic diseases in the general population during 2010 was: 32% for AR, 14% for AD, and 12% for asthma.20 Likewise, in our study including moderate to severe atopic population, the frequency of AR was 39.9% and of CARAS was 18.9%. Previously, authors have described the importance of AR in coexistence with asthma, as patients with uncontrolled AR symptoms may have an increased risk of asthma exacerbations.36 Therefore, controlling AR symptoms is particularly important in patients with CARAS. To date, allergen immunotherapy is mainly indicated for the treatment of moderate to severe AR, rather than exclusive asthma symptoms.16,22 However, current literature suggests that immunotherapy may improve asthma symptoms, decrease airway hyperresponsiveness, and lead to a reduction in medications.37 Besides, despite that the role of environmental allergens in triggering AD symptoms remains unclear, a current meta-analysis described that allergen immunotherapy can improve AD severity and quality of life.38 Therefore, as up to 15.63% of our study population presented a combination of the three main allergic diseases (AR, asthma, and AD), allergen immunotherapy may induce an immunological remission in these patients.39 Most of these studies have been performed in pediatric populations, and studies including adult populations, particularly in adults exposed to tropical environmental allergens (i.e., B. tropicalis), are needed.
The SPT findings in our population are consistent with the previously described distribution of allergens in patients undergoing immunotherapy in tropical and subtropical countries.40,41 Prior international studies have reported that the most common mites causing allergy in homes are house dust mites such as D. farinae. D. pteronyssinus, Euroglyphus maynei, and B. tropicalis.1,40 Up to 28.61% of the population had a positive SPT for B. tropicalis, which is particularly high considering that Bogota city has an oceanic climate with an average temperature of 14.5°C (58°F), average relative humidity of 75%, and a high altitude (2640 m or 8660 ft above sea level).42 Previous studies have suggested a higher prevalence of B. tropicalis in coastal cities with higher temperatures (over 18–27°C or 65–80°F) and humidity.43–45 However, over the last decades, an increase in sensitization rates to B. tropicalis has been reported.46 Current studies suggest that environmental variations induced by climate change and industrialization could partially explain the increase in the prevalence and severity of allergic disease, particularly in tropical countries.4 Additional studies assessing the changes in the prevalence of these tropical aeroallergens and the association between this prevalence and the changes in environmental conditions and climate change are needed.
Regarding the factors associated with exclusive AR, AR was most frequent in the population that reported a frequent acetaminophen consumption of more than four times a year (PR: 1.77; 95% CI: 1.12–2.25). Likewise, a current meta-analysis including observational studies by Zeng et al. among 87,0492 patients showed that the regular use of acetaminophen was related to a higher risk of AR symptoms (OR: 1.54; 95% CI: 1.41–1.69).47 Furthermore, a study conducted in a Colombian pediatric population described an association between AR and acetaminophen consumption over four times a year (PR: 1.31; 95% CI: 1.03–1.55).15 Different mechanisms could explain this association: (i) High doses of acetaminophen reduce levels of glutathione, an endogenous antioxidant in lung tissue, and increase pulmonary oxidative stress, causing progression of respiratory diseases48; (ii) COX-2 activity and increased prostaglandin E2 production could be stimulated by acetaminophen which promotes allergic pathways49; (iii) An IgE-mediated mechanism with acetaminophen as an antigenic agent.50–52 Moreover, several studies suggest that frequent use of acetaminophen may lead to a dose-dependent risk of developing allergic respiratory diseases, worsening lung function, and higher risk of respiratory diseases.51 However, due to the observational design of most of these studies, no causal relationship could be established, and this association may also reflect reverse causation because patients with a genetic predisposition to allergic diseases could be more prone to febrile syndromes due to respiratory tract infections and thus use acetaminophen more often. Overall, the evidence for this association has been stated in multiple observational studies, but further research is needed to assess this association. On the other hand, the authors highlight that additional medications were not explored in this study (i.e., antihistamines, antibiotics), as these assessments were not included in the original ISAAC-III questionnaire. However, further studies assessing the associations of the most frequently used medications in patients with allergies should be performed, as some observational studies have described these associations.53
On the other hand, CARAS was positively associated with cesarean delivery (PR = 1.44; 95% CI: 1.09 – 1.78). Similarly, a prior meta-analysis of observational studies by Darabi et al. stated that cesarean delivery increased the risk of childhood asthma (RR; 1.2; 95% CI: 1.15–1.25, P < 0.0001).54 A systematic review and meta-analysis assessing the pediatric consequences of cesarean section (C-section) revealed that C-section is a risk factor for asthma (pooled OR = 1.23 95% CI 1.14–1.33, P < 0.00001).55 A current meta-analysis assessing the association between cesarean delivery and childhood asthma also described a higher risk of asthma (OR = 1.26, 95% CI: 1.05–1.5) in children born by C-section.56 This association may be explained by different biological mechanisms such as changes in the immunological system development, changes in the infant microbiome, and the mechanical effects on lung growth that may lead to a higher neonatal respiratory morbidity.57 Despite the association between asthma and cesarean delivery seeming strong, the association between AR and cesarean delivery still has contradictory evidence.57,58 In a study by Richards et al., in a birth cohort of 117,768 children from the United States followed through 6 years of age, cesarean delivery was not associated with AR.58 However, Richards et al. reported that in this cohort children of mothers with allergies or asthma who underwent C-section were more likely to develop AR compared to children of mothers without allergies or asthma (AR-RR: 1.56; 95% CI: 1.46–1.67; AD-RR: 1.09; 1.00–1.19; food allergy RR: 1.31; 1.15–1.50); asthma RR: 1.31; 1.20–1.43).58 A meta--analysis by Bager et al. assessing the risk of cesarean delivery and risk of allergic diseases reported a higher risk of allergic rhinitis (OR 1.23, 95% CI 1.12–1.35; 7 studies), asthma (OR 1.18, 95% CI 1.05–1.32; 13 studies), and hospitalization for asthma (OR 1.21, 95% CI 1.12–1.31; 7 studies) in patients delivered via C-section.59 C-section babies are deprived of the first colonization of the gut with maternal vaginal bacteria and may exhibit a different gut flora compared with neonates born via vaginal delivery.59 The gut flora plays an important role in the homeostasis and development of the immune system, and C-sections could interfere with the normal tolerance induction and the homeostasis of the immune system, leading to a higher risk of atopic conditions. However, this meta--analysis highlights that a high heterogeneity was found between the studies due to major differences between the populations and methodology.59 Overall, this association may be explained by the relationships among different allergic diseases, but further studies are needed.
Despite no association being found, up to 31.5% of this atopic population were overweight or obese. This association between overweight status and atopy in pediatric populations has been described previously.60 Hersoug et al. hypothesized that obesity may decrease immunological tolerance due to changes induced in adipokines, cytokines, and tumor necrosis factor-alpha secreted by the adipose tissues.61 However, most of these studies were observational and only included pediatric populations. Further information regarding this interaction is needed to provide adult atopic patients with better care. Finally, this study highlights that the ISAAC-III questionnaire was useful to assess the factors associated with allergic diseases in adult populations, and further studies applying this standardized methodology should be performed.
A major limitation of this study was the observational methodological design that may show associations rather than prove causal relations among the variables.62 Moreover, as previously stated, all populations had a diagnosis of moderate to severe AR symptoms, and the population with mild symptoms of AR may have different associated factors. Among the strengths of the study, the diagnosis of allergic diseases was performed by allergists and confirmed with SPT following the EAACI guidelines.16 Thus, biases related to heterogeneity in clinical practice were avoided. Moreover, trained medical professionals with broad experience in the ISAAC-III questionnaire performed the data collection, following the ISAAC guidelines.9
Conclusion
A high frequency of B. tropicalis was found in this adult population aged 18–68 years with moderate to severe symptoms of AR confirmed with positive SPT undergoing immunotherapy. The main factor associated with AR was regular acetaminophen use, while the main factor associated with CARAS was cesarean delivery. These findings were consistent with previous reports in the scientific literature, and overall, the ISAAC-III questionnaire can be a useful low-cost tool to assess the factors associated with allergic diseases in tropical countries. Further studies assessing the factors associated with AR in tropical countries are needed.
Acknowledgments
We express our gratitude to the Universidad de Los Andes and the Department of Clinical Studies and Epidemiology of the Fundación Santa Fe de Bogotá. We also thank all the allergists who supported the fieldwork of this study.
Conflict of Interest
The authors declare that they have no conflicts of interest.
Funding
This work was supported by UNIMEQ-ORL, Bogotá, Colombia.
REFERENCES
1. Caraballo L, Zakzuk J, Lee BW, Acevedo N, Soh JY, Sánchez-Borges M, et al. Particularities of allergy in the tropics. World Allergy Org J [Internet]. 2016;9:20. 10.1186/s40413-016-0110-7
2. Haahtela T, Holgate S, Pawankar R, Akdis CA, Benjaponpitak S, Caraballo L, et al. The biodiversity hypothesis and allergic disease: World allergy organization position statement. World Allergy Org J. 2013;6:3. 10.1186/1939-4551-6-3
3. Moreno-López S, Pérez-Herrera LC, Peñaranda D, Hernández DC, García E, Peñaranda A. Prevalence and-associated factors of allergic diseases in school children and-adolescents aged 6-7 and 13-14 years old from two rural areas in Colombia. Allergol Immunopathol (Madr). 2021;49:153–161. 10.15586/aei.v49i3.183
4. Acevedo N, Zakzuk J, Caraballo L. House dust mite allergy under changing environments. Allergy Asthma Immunol Res. 2019;11:450. 10.4168/aair.2019.11.4.450
5. Pinto Pereira LM, Jackman J, Figaro N, Babootee N, Cudjoe G, Farrell S, et al. Health burden of co-morbid asthma and allergic rhinitis in West Indian children. Allergol Immunopathol (Madr). 2010;38:129–134. 10.1016/j.aller.2009.09.002
6. Bousquet J, Schünemann HJ, Samolinski B, Demoly P, Baena-Cagnani CE, Bachert C, et al. Allergic Rhinitis and its Impact on Asthma (ARIA): Achievements in 10 years and future needs. J Allergy Clin Immunol. 2012;130:1049–62. 10.1016/j.jaci.2012.07.053
7. Pearce N, Aït-Khaled N, Beasley R, Mallol J, Keil U, Mitchell E, et al. Worldwide trends in the prevalence of asthma symptoms: Phase III of the International Study of Asthma and Allergies in Childhood (ISAAC). Thorax. 2007; 10.1136/thx.2006.070169
8. Pols DHJ, Wartna JB, Alphen EI van, Moed H, Rasenberg N. Interrelationships between atopic din children: A meta--analysis based on ISAAC questionnaires. 2015;1–15. 10.1371/journal.pone.0131869
9. Asher MI, Montefort S, Björkstén B, Lai CK, Strachan DP, Weiland SK, et al. Worldwide time trends in the prevalence of symptoms of asthma, allergic rhinoconjunctivitis, and eczema in childhood: ISAAC phases one and three repeat multicountry cross-sectional surveys. Lancet. 2006;368:733–43. 10.1016/S0140-6736(06)69283-0
10. Barbarot S, Auziere S, Gadkari A, Girolomoni G, Puig L, Simpson EL, et al. Epidemiology of atopic dermatitis in adults: Results from an international survey. Allergy. 2018;73:1284–93. 10.1111/all.13401
11. Frati F, Incorvaia C, Cavaliere C, di Cara G, Marcucci F, Esposito S, et al. The skin prick test. J Biol Regul Homeost Agents. 2018;32(1 Suppl. 1):19–24.
12. Heinzerling L, Mari A, Bergmann K-C, Bresciani M, Burbach G, Darsow U, et al. The skin prick test – European standards. Clin Transl Allergy. 2013. p. 3.
13. Kim B-J, Mun S-K. Objective measurements using the skin prick test in allergic rhinitis. Arch Otolaryngol Head Neck Surg. 2010;136:1104–1106. 10.1001/archoto.2010.185
14. Tschopp JM, Sistek D, Schindler C, Leuenberger P, Perruchoud AP, Wuthrich B, et al. Current allergic asthma and rhinitis: Diagnostic efficiency of three commonly used atopic markers (IgE, skin prick tests, and Phadiatop). Results from 8329 randomized adults from the SAPALDIA Study. Swiss Study on Air Pollution and Lung Diseases in Adults. Allergy. 1998;53:608–13. 10.1111/j.1398-9995.1998.tb03937.x
15. Peñaranda A, Gantiva M, Moreno-López S, Peñaranda D, Perez-Herrera LC, Garcia E. Factors associated with allergic rhinitis and combined allergic rhinitis and asthma syndrome (CARAS) in children aged 5–18 years undergoing immunotherapy in a tropical low-or middle-income country. Allergol Immunopathol (Madr). 2023;51:126–32. 10.15586/aei.v51i1.509
16. Roberts G, Pfaar O, Akdis CA, Ansotegui IJ, Durham SR, Gerth van Wijk R, et al. EAACI Guidelines on allergen immunotherapy: Allergic rhinoconjunctivitis. Allergy. 2018;73:765–98. 10.1111/all.13317
17. Alvaro-Lozano M, Akdis CA, Akdis M, Alviani C, Angier E, Arasi S, et al. EAACI allergen immunotherapy user’s guide. Pediatr Allergy Immunol. 2020 May;31(25):1–101. 10.1111/pai.13189.
18. Mortuaire G, Michel J, Papon JF, Malard O, Ebbo D, Crampette L, et al. Specific immunotherapy in allergic rhinitis. Eur Ann Otorhinolaryngol Head Neck Dis [Internet]. 2017;134:253–258. 10.1016/j.anorl.2017.06.005
19. Dennis RJ, Caraballo L, García E, Rojas MX, Rondon MA, Pérez A, et al. Prevalence of asthma and other allergic conditions in Colombia 2009–2010: A cross-sectional study. BMC Pulm Med. 2012;12:17. 10.1186/1471-2466-12-17
20. Pérez-Herrera LC, Moreno-López S, Peñaranda D, García E, Chapman E, Peñaranda A. Frequency of self-reported allergies at a high-complexity referral hospital in Colombia, a tropical Latin American country. Allergol Immunopathol (Madr). 2021;49:100–5 10.15586/aei.v49i5.449
21. Paiva Ferreira LKD, Paiva Ferreira LAM, Monteiro TM, Bezerra GC, Bernardo LR, Piuvezam MR. Combined allergic rhinitis and asthma syndrome (CARAS). Int Immunopharmacol. 2019;74:105718. 10.1016/j.intimp.2019.105718
22. Papadopoulos NG, Agache I, Bavbek S, Bilo BM, Braido F, Cardona V, et al. Research needs in allergy: An EAACI position paper, in collaboration with EFA. Clin Transl Allergy [Internet]. 2012;2:21. 10.1186/2045-7022-2-21
23. DANE. Censo Nacional de Poblacion y Vivienda 2018 Colombia. 2018., Dirección de Censos y Demografía: Bogotá, Colombia.
24. Mata Fernández C, Fernández-Benítez M, Pérez Miranda M, Guillén Grima F. Validation of the Spanish version of the Phase III ISAAC questionnaire on asthma. J Investig Allergol Clin Immunol. 2005;15:201–10.
25. Kim DH, Lim DH, Samra M, Kim EH, Kim JH. How accurate are the ISAAC questions for diagnosis of allergic rhinitis in Korean children? Int J Environ Res Public Health [Internet]. 2018;15:1527. 10.3390/ijerph15071527
26. Beasley RW, Clayton TO, Crane J, Lai CKW, Montefort SR, Mutius E von, et al. Acetaminophen use and risk of asthma, rhinoconjunctivitis, and eczema in adolescents. Am J Respir Crit Care Med. 2011;183:171–8. 10.1164/rccm.201005-0757OC
27. World Health Organization. Body Mass Index [Internet]. WHO library. 2018 [cited
28. Schiaffino A, Rodriguez M, Pasarin MI, Regidor E, Borrell C, Fernandez E. Odds ratio or prevalence ratio? Their use in cross-sectional studies. GacSanit. 2003;17:70–4. 10.1157/13043426
29. Thompson M Lou, Myers JE, Kriebel D. Prevalence odds ratio or prevalence ratio in the analysis of cross sectional data: What is to be done? Occup Environ Med. 1998;55:272–7. 10.1136/oem.55.4.272
30. Mims JW. Epidemiology of allergic rhinitis. Int Forum Allergy Rhinol. 2014;4:18–20. 10.1002/alr.21385
31. Sánchez J, Sánchez A. Epidemiologic studies about food allergy and food sensitization in tropical countries. Results and limitations. Allergol Immunopathol (Madr). 2019;47:401–408. 10.1016/j.aller.2018.11.001.
32. Pearce N, Sunyer J, Cheng S, Chinn S, Björkstén B, Burr M, et al. Comparison of asthma prevalence in the ISAAC and the ECRHS. Eur Respir J. 2000;16:420–6. 10.1183/9031936.00.16337700
33. Acharya KP, Pathak S. Applied research in low-income-countries: Why and how? Front Res Metr Anal. 2019;4:3. 10.3389/frma.2019.00003
34. Helmy M, Awad M, Mosa KA. Limited resources of genome sequencing in developing countries: Challenges and solutions. Appl Transl Genom. 2016;9:15–9. 10.1016/j.atg.2016.03.003
35. Gaillard J. Measuring research and development in developing countries. Sci Technol Society. 2010;15:77–111. 10.1177/097172180901500104
36. Bousquet J. Allergic rhinitis and its impact on asthma (ARIA) 2008. Allergy. 2008;63:1052–5. 10.1111/j.1398-9995.2007.01620.x
37. Nakagome K, Nagata M. Allergen immunotherapy in asthma. Pathogens. 2021;10:1406. 10.3390/pathogens10111406
38. Yepes-Nuñez JJ, Guyatt GH, Gómez-Escobar LG, Pérez-Herrera LC, Chu AWL, Ceccaci R, et al. Allergen immunotherapy for atopic dermatitis: Systematic review and meta-analysis of benefits and harms. J Allergy Clin Immunol. 2023;151:147–58. 10.1016/j.jaci.2022.09.020
39. Nagata M, Nakagome K. Allergen immunotherapy in asthma: Current status and future perspectives. Allergol Int. 2010;59:15–9. 10.2332/allergolint.09-RAI-0150
40. Devillier P, Dreyfus J-F, Demoly P, Calderón MA. A meta-analysis of sublingual allergen immunotherapy and pharmacotherapy in pollen-induced seasonal allergic rhinoconjunctivitis. BMC Med [Internet]. 2014;12:71. 10.1186/1741-7015-12-71
41. Bousquet J, Schünemann HJ, Togias A, Bachert C, Erhola M, Hellings PW, et al. Next-generation allergic rhinitis and its impact on asthma (ARIA) guidelines for allergic rhinitis based on grading of recommendations assessment, development and evaluation (GRADE) and real-world evidence. J Allergy Clin Immunol [Internet]. 2020;145:70–80.e3. 10.1016/j.jaci.2019.06.049
42. Institute of Hydrology, Meteorology and Environmental Studies I. Colombian average climate annual report [Internet]. Bogota, Colombia; 2019. Available from: http://www.ideam.gov.co/documents/21021/553571/Promedios+Climatológicos++1981+-+2010.xlsx/f28d0b07-1208-4a46-8ccf-bddd70fb4128
43. Puerta L, Fernandez E, Mercado D, Lockey R, Caraballo L. Sequential determinations of. J Allergy Clin Immunol. 1996;97:689–91. 10.1016/S0091-6749(96)70315-9
44. Luis AC, Gloria G, Dary MM, Eduardo EB. Standardization and establishment of an in vitro culture of Blomia tropicalis toward technological development purposes. Front Immunol. 2015;6:1–2. 10.3389/conf.fimmu.2015.05.00264
45. Stewart GA, Robinson C. Indoor and outdoor allergens and pollutants. In: O'Hehir R, Holgate S, Hershey GK, Sheikh A, editors. Middleton’s allergy essentials. Elsevier: Philadelphia, USA; 2017. p. 73–116.
46. Jeevarathnum AC, van Niekerk A, Green R, Becker P, Masekela R. Prevalence of Blomia tropicalis allergy in two regions of South Africa. South African Medical Journal. 2015;105:567. 10.7196/SAMJnew.7786
47. Zeng Y, Song B, Gao Y, Cao W, Li J, Liu Q, et al. Cumulative evidence for association of acetaminophen exposure and allergic rhinitis. Int Arch Allergy Immunol. 2020;181:422–33. 10.1159/000506807
48. Dröge W, Breitkreutz R. Glutathione and immune function. Proc Nutr Soc. 2000;59:595–600. 10.1017/S0029665100000847
49. Swierkosz TA, Jordan L, McBride M, McGough K, Devlin J, Botting RM. Actions of paracetamol on cyclooxygenases in tissue and cell homogenates of mouse and rabbit. Med Sci Monit. 2002;8:BR496–503.
50. Wang J-Y, Liu L-F, Chen C-Y, Huang Y-W, Hsiung CA, Tsai H-J. Acetaminophen and/or antibiotic use in early life and the development of childhood allergic diseases. Int J Epidemiol. 2013;42:1087–99. 10.1093/ije/dyt121
51. Allmers H. Frequent acetaminophen use and allergic diseases: Is the association clear? J Allergy Clin Immunol. 2005;116:859–62. 10.1016/j.jaci.2005.07.019
52. Paramo BJ, Gancedo SQ, Cuevas M, Camo IP, Martin JA, Cosmes EL. Paracetamol (acetaminophen) hypersensitivity. Ann Allergy Asthma Immunol. 2000;85:508–11. 10.1016/S1081-1206(10)62580-X
53. Kawauchi H, Yanai K, Wang D-Y, Itahashi K, Okubo K. Antihistamines for allergic rhinitis treatment from the viewpoint of nonsedative properties. Int J Mol Sci. 2019;20:213. 10.3390/ijms20010213
54. Darabi B, Rahmati S, HafeziAhmadi MR, Badfar G, Azami M. The association between caesarean section and childhood asthma: An updated systematic review and meta-analysis. Allergy Asthma Clin Immunol. 2019;15:62. 10.1186/s13223-019-0367-9
55. Słabuszewska-Jóźwiak A, Szymański JK, Ciebiera M, Sarecka-Hujar B, Jakiel G. Pediatrics consequences of caesarean-section—A systematic review and meta-analysis. Int J Environ Res Public Health. 2020;17:8031. 10.3390/ijerph17218031
56. Wypych-Ślusarska A, Niewiadomska E, Oleksiuk K, Krupa-Kotara K, Głogowska-Ligus J, Słowiński J. Caesarean delivery and risk of childhood asthma development: Meta-analysis. Postepy Dermatol Alergol. 2021;38:819–26. 10.5114/ada.2020.96703
57. Maitra A, Sherriff A, Strachan D, Henderson J. Mode of delivery is not associated with asthma or atopy in childhood. Clin Exp Allergy. 2004;34:1349–55. 10.1111/j.1365-2222.2004.02048.x
58. Richards M, Ferber J, Li D-K, Darrow LA. Cesarean delivery and the risk of allergic rhinitis in children. Ann Allergy Asthma Immunol. 2020;125:280–286.e5. 10.1016/j.anai.2020.04.028
59. Bager P, Wohlfahrt J, Westergaard T. Caesarean delivery and risk of atopy and allergic disesase: meta-analyses. Clin Exp Allergy. 2008;38:634–42. 10.1111/j.1365-2222.2008.02939.x
60. Yoo S, Kim H-B, Lee S-Y, Kim B-S, Kim J-H, Yu J-H, et al. Association between obesity and the prevalence of allergic diseases, atopy, and bronchial hyperresponsiveness in Korean adolescents. Int Arch Allergy Immunol. 2011;154:42–8. 10.1159/000319207
61. Hersoug L-G, Linneberg A. The link between the epidemics of obesity and allergic diseases: Does obesity induce decreased immune tolerance? Allergy. 2007;62:1205–13. 10.1111/j.1398-9995.2007.01506.x
62. Tamhane AR, Westfall AO, Burkholder GA, Cutter GR. Prevalence odds ratio versus prevalence ratio: Choice comes with consequences. Stat Med. 2016;35:5730–5. 10.1002/sim.7059