
Download
ORIGINAL ARTICLE
Early life triggers for food allergy that in turn impacts dietary habits in childhood
Emilia Vassilopouloua*, Elisabeth Vardakaa, Dimitris Efthymioub, Constantinos Pitsiosc
aDepartment of Nutritional Sciences and Dietetics, School of Health Sciences, International Hellenic University, Thessaloniki, Greece
bUniversity Psychiatric Clinic, Department of Psychiatry, Division of Neuroscience, Medical School, Aristotle University of Thessaloniki, Thessaloniki, Greece
cMedical School, University of Cyprus, Nicosia, Cyprus
Abstract
Introduction and objectives: In order to investigate food allergy’s prevalence, risk factors and eating behavior of children with relevant anamnesis, a study was performed in Cypriot primary schools.
Patients: A specially composed questionnaire for self-reported adverse reactions to food, created in the context of the EuroPrevall study, was distributed in 13 representative primary schools across the country. Participants were sub-grouped into three groups; healthy (H), those with unconfirmed food hypersensitivity reactions (FA-) and children with a confirmed diagnosis by a physician IgE-mediated food allergy (FA+). Food habits, family health history and lifestyle factors were assessed and groups’ outcomes were compared with each other.
Results: For the study, 202 questionnaires were completed and returned; 31 children (19 FA- and 12 FA+) reported an adverse food reaction. Significant risk factors for developing FA+ were being the first born or having siblings with asthma, attended a day nursery, but also maternal alcohol drinking during pregnancy, parental smoking and parental occupation in food processing or use of latex gloves. The presence of children in the kitchen during cooking showed a protective role. Dietary habits of FA+ children were significantly diminished in terms of variety and frequency of consumption in comparison to the rest, in which had a greater overlap.
Conclusion: Further research is required for the interesting risk or protective factors revealing from the current investigation. The negative effect of food allergy in the dietary habits of food allergic children documented in the literature, is strongly supported herein.
Key words: breast-feeding, food allergy, food consumption, food hypersensitivity, parental smoking
*Corresponding author: Emilia Vassilopoulou, Department of Nutritional Sciences and Dietetics, School of Health Sciences, International Hellenic University, Alexander Campus, Thessaloniki, 574 00, Greece. Email address: [email protected]
Received 21 January 2021; Accepted 29 January 2021 Available online 1 May 2021
Copyright: Vassilopoulou E, et al.
License: This open access article is licensed under Creative Commons Attribution 4.0 International (CC BY 4.0). http://creativecommons.org/licenses/by/4.0/
Introduction
Food allergy prevalence during the last decades increases in parallel to other atopic diseases, especially in industrialized countries, reaching 6% in Europe, USA, and Canada.1–3 However, estimates of food allergy prevalence vary widely among studies, likely due to genetic and epigenetic factors of the studied populations, maternal diet in pregnancy and breastfeeding, mode of delivery, infant feeding practices, different eating habits, and environmental factors such as climate, flora, exposure to sun, and air pollution.4–7
Study methodologies assessing food allergy prevalence are leading to high differences among studies.8 For example, outcomes based on data recruited with self- or parent- reported questionnaires, contacted by mails, by interviews or on-line, might show high discrepancy with the ones based on medically confirmed diagnosis of food allergy.2,9
Food allergy is a common problem, especially in children. The best way to prevent food allergic exacerbation symptoms is to avoid the culprit food. Nevertheless, the concern of physicians, dietitians, and nutritionists is that extended avoidance of foods may lead to many complications, such as unbalanced diet, poor nutrition, failure to thrive, protein losing enteropathy, hypocalcemic seizures and rickets.10 Additionally, quality of life is significantly affected, due to the food restrictions and the emotional impact on patients arising from anxiety and social limitations.11
Based on the high heterogeneity of food allergy among South and North European countries and the limited available data of food allergy in Cyprus, the current study aimed to detect the prevalence and risk factors of self-reported hypersensitivity reactions to food and food allergies, as well as to evaluate the impact of these reactions on their dietary habits.
Materials and Methods
Participants
A community-based survey was performed with the recruitment of children from 13 representative primary schools from both urban and rural areas of Cyprus, with stratified random sampling. Information was collected through a specially composed questionnaire for self-reported adverse reactions to food, created in the context of the EuroPrevall study.12–14
3000 typed questionnaires were distributed in children, after being translated with standardized translation procedures, including forward (from English to Greek) and backward translation (comparison and necessary editing) and pilot use of the questionnaires, and filled by parents or caregivers, together with a signed informed consent.14
The study was approved by the Cypriot Bioethics Committee, the Department of Education of Cyprus’ Ministry of Education.
Surveyed information
The questionnaire was a comprehensive tool, containing different groups of questions. The first group of questions included information regarding gestation, mode and conditions of delivery, birth weight and height and mother’s age at delivery, short (≤4 months) breast-feeding duration, age of formula introduction, birth order trait in the family, use of antibiotics during the first 2 years of life, age of first attendance in a day nursery and room sharing with siblings.
The second group of questions focused on the history of food adverse reactions, including description of symptoms, time of onset, confirmed diagnosis by a physician confirmation with relevant skin prick tests (SPT) and/or blood tests. Additional information regarding the eating habits were recorded depicting information regarding dietary variety, food frequency consumption, and food supplement use.
The third group of questions aimed to collect information regarding the family history of food allergy and/or atopy. Information regarding parental lifestyle recorded were smoking during pregnancy and breastfeeding, maternal alcohol use during pregnancy, parental occupation related to food processing, use of latex gloves at work, and children’s presence in the kitchen during cooking.
Statistical analysis
All continuous variables were transformed to achieve normality.15 Shapiro–Wilk Test was used to determine the normality of data at 0.05 significant level. Student’s t-test was performed to examine the statistical significance of mean’s variation between genders. Analysis of variance (ANOVA) followed by a multiple comparison test (Tamhane post-hoc test) was assessed to examine the statistical significance of mean’s variation among study groups.16 Chi-squared test (χ2-test) was performed to associate categorical variables. Discriminant analysis was used to distinguish differences on food frequency consumption among study groups.16 The accuracy of the grouped cases classification was examined using cross-validation through the leave-one-out method. Significant relationships were defined as p < 0.05 and very significant as p < 0.001. The statistical data analysis was performed using SPSS 17.0.
Results
Participants’ characteristics
For the study, 202 fully completed (response rate 6.7%) questionnaires were finally included in the analysis. Approximately, equal number of boys and girls returned the questionnaires (Table 1). The age of children ranged from 5.5 to 12 years (8.7 ± 1.7 years), with no significant difference in the mean age among boys and girls (t-test, p > 0.05), and similar gender distribution among different age groups (χ2 = 0.633, p > 0.05).
Table 1 Distribution of children (number and percentage) that participated in the study, by age and gender.
| Age (years) | Boys | Girls | Total |
|---|---|---|---|
| 5–7 | 27 (25.2%) | 28 (29.5%) | 55 (27.2%) |
| 8–9 | 39 (36.49%) | 35 (36.8%) | 74 (36.6%) |
| 10–12 | 41 (38.3%) | 32 (33.7%) | 73 (36.1%) |
| Total | 107 (100%) | 95 (100%) | 202 (100%) |
Further, 31 children (15.3%) reported at least one episode of “discomfort” or “disorder” caused by food consumption and these were considered as food hypersensitivity reactions (FHR). The onset of an FHR was reported at a mean age of 3.3 years (SD = ±2.2, min = 2, max = 9). FHR were experienced 1.6 times more frequently in girls than in boys (19 vs 12). Among the children reporting an FHR, 12 had a confirmed diagnosis of food allergy.
An apriori grouping was not only used to distinguish healthy children from the ones with anamnesis of FHR, but also self-reported from medically confirmed food allergy. Children were grouped as healthy, without food sensitivities (H, NH = 171, NH♂ = 95), those with unconfirmed FHR (FA-, NFA- = 19, N FA-♂ = 4), and those with confirmed diagnosis of food allergy (FA+, NFA+ = 12, N FA+♂ = 8), (Table 3).
Table 2 Foods reported: (a) to cause an adverse reaction and (b) to be avoided by the children.
| Food | Food allergic children | |||||
|---|---|---|---|---|---|---|
| With an illness or a disorder caused after eating a food or foods (N= 31, N♂ = 12, NFA+ = 12) | Avoiding a food or several foods because they make them feel ill (N = 22, N♂ = 7, NFA+ = 8) | |||||
| N | ♂ (%) | FA+ (%) | N | ♂ (%) | FA+ (%) | |
| Vegetables and legume | ||||||
| Celery | 1 | 100 | 0 | 1 | 100 | 0 |
| Tomato* | 7 | 57 | 43 | 1 | 0 | 0 |
| Carrot | 2 | 100 | 100 | – | – | – |
| Lentil | 3 | 67 | 67 | 1 | 0 | 0 |
| Soya | 4 | 50 | 100 | 4 | 50 | 100 |
| Chickpeas | 2 | 50 | 0 | 2 | 50 | 0 |
| Seeds | ||||||
| Sesame seeds | 6 | 67 | 83 | 5 | 60 | 100 |
| Sunflowers seeds | 2 | 100 | 100 | – | – | – |
| Mustard | 3 | 33 | 100 | 1 | 100 | 100 |
| Poppy seeds | 4 | 50 | 100 | 4 | 50 | 100 |
| Pine seeds | 1 | 0 | 0 | 1 | 0 | 0 |
| Fruits & berries | ||||||
| Apples | 1 | 0 | 0 | 1 | 0 | 0 |
| Bananas* | 4 | 50 | 25 | 2 | 50 | 50 |
| Kiwifruit | 1 | 0 | 0 | 1 | 0 | 0 |
| Peach | 1 | 100 | 100 | – | – | – |
| Strawberry* | 1 | 100 | 0 | 1 | 100 | 0 |
| Cow’s milk* | 9 | 33 | 33 | 6 | 33 | 33 |
| Nuts | ||||||
| Hazelnut* | 1 | 0 | 100 | 1 | 0 | 100 |
| Peanut | 1 | 0 | 100 | 1 | 0 | 100 |
| Walnut | 1 | 0 | 100 | 1 | 0 | 100 |
| Cereal | ||||||
| Wheat* | 5 | 60 | 100 | 1 | 100 | 100 |
| Rice | 2 | 100 | 100 | – | – | – |
| Buckweat | 2 | 0 | 100 | – | – | – |
| Chocolate | 2 | 50 | 50 | 2 | 50 | 50 |
| Egg | 6 | 33 | 67 | 4 | 0 | 50 |
| Fish | 5 | 40 | 20 | 4 | 25 | 25 |
| Total responses | 77 | 45 | ||||
*Foods causing the most serious reactions.
Table 3 Age of mother and child during delivery, child’s height and weight at birth (N = number of relative provided data).
| N | Mean | SD | Min | Max | ||
|---|---|---|---|---|---|---|
| Mother’s age during pregnancy (years) | H | 141 | 29.2 | 5.1 | 18 | 42 |
| FA- | 17 | 28.1 | 4.6 | 20 | 35 | |
| FA+ | 12 | 28.4 | 5.7 | 20 | 35 | |
| Total | 170 | 29.0 | 5.1 | 18 | 42 | |
| Duration of gestation (months) | H | 171 | 8.6 | 1.7 | 5.5 | 11.9 |
| FA- | 19 | 8.7 | 1.6 | 6.4 | 12.1 | |
| FA+ | 12 | 9.2 | 1.8 | 6.0 | 11.8 | |
| Total | 202 | 8.7 | 1.7 | 5.5 | 12.1 | |
| Height at birth (cm) | H | 113 | 50.4 | 3.9 | 30 | 67 |
| FA- | 14 | 48.9 | 4.4 | 38 | 53 | |
| FA+ | 4 | 49.5 | 1.3 | 48 | 51 | |
| Total | 131 | 50.2 | 3.9 | 30 | 67 | |
| Weight at birth (grams) | H | 132 | 3135.6 | 591.3 | 1000 | 4450 |
| FA- | 15 | 3123.0 | 410.8 | 2150 | 3650 | |
| FA+ | 9 | 3190.0 | 456.0 | 2650 | 3850 | |
| Total | 156 | 3137.5 | 567.1 | 1000 | 4450 | |
In 30/31 children reporting FHR, symptoms occurred during the first hour after consumption (mean time = 20 min), while in 12 cases, they occurred 24 h later. Symptoms mainly involved skin (with rash and/or eczema) in 90% of the cases, the gastrointestinal tract (reporting diarrhea, vomiting, or abdominal pain) in 53% of the cases and upper airways in 20% of the cases
Among the 32 foods included in the used questionnaire (Table 2), 26 were implicated in a reported FHR. Cow’s milk was the most frequently offending food, followed (in decreasing order) by tomato, eggs, and sesame seeds (Table 2). On an average, 6.2 and 3.8 foods were reported to cause symptoms in FA+ and FA- groups, respectively. Differences of the culprit foods were noticed between girls and boys. Only girls implicated nuts as the cause of FHR and they also incriminated cow’s milk more frequently than boys. On the contrary, rice was exclusively implicated in food reaction by boys, who also reported sesame as a culprit food more often than girls.
Personal or familial factors implicated to FHR
No significant variations were noticed for gestational duration (8.7 ± 1.7 months), birth weight (3137.5 ± 567.1 g), and birth height (50.2 ± 3.9 cm) between the three study groups and no effect of mother’s age at delivery was either noticed (ANOVA, p > 0.05) (Table 3). No statistically significant difference between groups was registered regarding shorter than 4 months breast-feeding, or for the use of antibiotics during the first 2 years of life (Table 4).
Table 4 Risk factors of food adverse reactions in children.
| Risk factor | H (%) N = 151 | FA- (%) N = 19 | FA+ (%) N = 12 |
|---|---|---|---|
| Short duration of breast-feeding (≤4 mon.) | 67 (39.2) | 6 (31.6) | 6 (50) |
| Antibiotics in the first 2 years of life – NAI | 90 (52.6) | 8 (42.1) | 7 (58.3) |
| Mother smoking and/or drank alcohol during pregnancya | 18 (10.5) | 0 | 5 (41.7)** |
| Day nursery | 41 (24.0) | 5 (26.3) | 7 (58.3)* |
| Children shared their room with siblings | 44 (25.7) | 5 (26.3) | 7 (58.3) |
| Family anamnesis of atopy (allergic eczema, allergic rhinitis/rhinoconjunctivitis, asthma) | 81 (47.4) | 9 (47.5) | 5 (41.7) |
| Family anamnesis of atopy + food allergy | 81 (47.4) | 10 (52.6) | 8 (66.7) |
| Any family smoking during first 2 years of life | 34 (15.9) | 5 (26.3) | 6 (50)* |
| Any parent with food allergy | 20 (13.2) | 3 (15.7) | 4 (33)* |
| Any parent work related to food processing | 25 (14.6) | 5 (26.3) | 6 (50.0)* |
| Any parent using latex gloves at work | 51 (29.8) | 5 (26.3) | 6 (50.0) |
χ2 test: *p< 0.05, **p < 0.001.
aχ2 test perform between healthy and FA+ groups.
FA+ children attended a day nursery at a younger age (χ2 = 7.165, p < 0.05) compared with other groups and were the first-born of the family, while most FA- were more often the second born. Despite that the comparison of familial anamnesis of allergy did not differ significantly among groups, anamnesis of food allergy as an independent parameter, was significantly higher in the FA+ group (33%) than in the H and FA- ones (13.2% and 15.7%, respectively). More than 50% of the FA+ children shared their room with siblings, whereas only 25–27% of children from other groups had to share their room.
Maternal smoking during pregnancy (average 15 cigarettes daily) and alcohol consumption (frequency/quantity undefined) were significantly higher in the FA+ group. Similarly, parental smoking during the first 2 years of life was found significantly higher than in the other two groups.
Noteworthy, parental occupation related to food processing was found to significantly increase the risk for the development of food allergy in our study population (Table 4). The use of latex gloves was similar in H and FA+ groups. Direct exposure of children to food processing during cooking was also examined as a putative sensitizing or protective factor. It was observed that mostly healthy and FA- children were more often or occasionally in the kitchen during cooking than FA+ children.
Frequency of food consumption and food habits
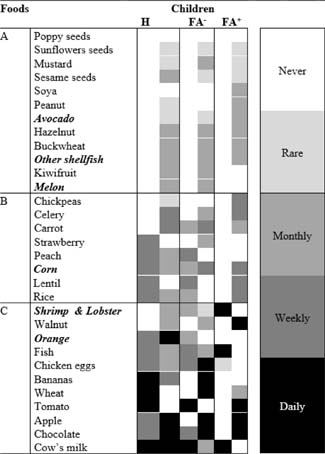
Based on the answers of the food frequency questions, a heatmap was prepared to visualize children’s food choices (Figure 1). Foods were distributed in a scale reflecting the increasing frequency of food consumption (A to C) among children (Figure 1). Subgroup A included foods rarely or never consumed by the majority of children, subgroup B included foods with a moderate consumption (≤once weekly), while subgroup C included foods with the highest consumption (more than once a week or daily).
Figure 1 Heatmap of the frequency of food consumption among Healthy (H; N = 151) and children with a food adverse reaction without (FA-; N = 17) or with (FA+; N = 10) a food allergy diagnosis. For each food the predominant (>70%), or the first two dominant (in total >60%) frequency categories in ordinal scale (Never to Daily) are given. With bold are indicated foods not implicated in adverse reactions.
Cow’s milk was an abundant food (>70%) in all children’s diet. Semi-fat milk was usually consumed by the healthy and FA- (67% and 50%, respectively), whereas the FA+ usually consumed full fat or semi-fat milk (42% each type). A minority of children had used vitamin D supplement (H = 18.7% FA+ = 8.3%, FA- = 5.3%).
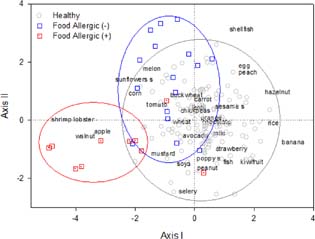
A discriminant analysis was performed to determine the children’s dietary choices among the three study groups. The analysis indicates that differences among groups can be found along two canonical linear discriminant functions (Axis I and II). Figure 2 shows the spatial positions of the three study groups with respect to the two Axes arising from the analysis, as well as the contribution of the consumption frequency of each food (discriminating variables) to the formation of the Axis. Best differential variables occupy positions furthest from the center of the ordination field (e.g. banana, shrimp and lobster, shellfish) while non-differential variables mainly occupy positions near the origin and are not indicative of any particular distinguishing characteristic (e.g. orange, wheat).
Figure 2 Ordination of the discriminant analysis for the three children’s groups, based on the frequency of the consumption of each food. The foods are not represented by arrows for readability of the diagram.
Discriminating variables which are in close proximity indicate significant positive correlations between the variables (e.g. apple, walnut), while those diagonally opposite indicate significant negative correlations (e.g. walnut, hazelnut).
Axis I which accounts for 68% of the discriminating ability of the variables, differentiates FA+ group from the other two groups. The major differences were that FA+ children are characterized by a relative higher consumption of foods such as shrimp and lobster, walnut, and apple and a relative lower consumption of foods such as banana, hazelnut, rice, kiwifruits, peaches, and eggs.
FA- children appear to have similar food choices with H children, as indicated by the significant overlap. FA- group differentiated from H group along Axis II, which accounts for 32% of the discriminating ability of the variables. The major differences between the FA- group and the H group were that FA- group is characterized by a relative higher consumption of foods such as shellfish, egg, melon, sunflower seeds, and relatively lower consumption of foods such as celery, peanut, and fish.
Discriminant analysis showed adequate sensitivity and specificity: 80% of the children of FA+ group, 77% of FA- group, and 83% of H group were correctly identified. However, using the cross-validation through the leave-one-out method, the classification efficiency of each group showed higher error rate. The classification function had lower but decent success classifying cases in groups FA+ (70%) and H (72%) whereas in FA- group, the results were highly undistinguishable (41%).
Discussion
In the current study, the rate of reported FHR in Cypriot elementary pupils was 15.3%, while 5.9% of the enrolled children had anamnesis of confirmed food allergy. Our findings are in line with previous reports in Southern Europe (8.6%) and slightly lower than in Italy (10.5%), that is also in the Mediterranean area.17,18 Our data are in accordance with the notion that the life-time prevalence of self-reported food allergy is extremely lower in Southern Europe than in Western (23.8%), Northern (30.3%), and Eastern Europe (41.6%).17
An interesting remark is that 81.25% of the foods included in the questionnaire were implicated in reported FHR, with cow’s milk, wheat, strawberry, banana, and tomato causing the most severe reactions. Although food allergy was not confirmed in all cases of FHR, in 97% of them symptoms occurred during the first hour after food consumption and persisted for approximately 1 h, increasing the possibility that an IgE-mediated food allergic reaction had occurred.
Our findings confirm results from a former study regarding differences between healthy and food allergic pupils of Cypriot primary schools; using two 24-h recalls, a lower energy intake and an overall lower nutrient consumption were shown in children with self-reported food allergy.14 They reported unhealthier food choices than their peers, while their diet was monotonous, avoiding the combination of foods from different groups and they reported low consumption of milk, dairy products, fiber, vegetable oils, and whole-wheat bread.14
In food allergic children, elimination diets are suggested for a limited period, in order to outgrow allergy. Food avoidance is reported to affect eating habits, leading to food neophobia and pickiness.19 Additionally, parental and social influence have significant impact in developing food neophobia.20,21 As expected, in our study, children with confirmed diagnosis of food allergy were shown to be more “picky eaters” than healthy children.
Interestingly, a high differentiation of dietary behavior was noticed among FA+ and FA- children, while eating habits of FA- and healthy children were highly overlapping. A possible hypothesis explaining this observation is that children of the FA+ group were strictly avoiding one or more foods, after the food allergy diagnosis by a physician and this had impacted the variety of their diet.
Heredity is considered as one of the main risk factors for the development of food allergy and other allergic diseases.4,22,23 Parent’s anamnesis of food allergy was confirmed as a risk factor in our study population, whereas anamnesis of other atopic diseases appeared irrelevant. On the other hand, breast-feeding duration was similar in the three groups so a potential protective effect for food allergy was not determined herein. Although breast-feeding reduces the risk for diseases of the gastrointestinal tract, infections, atopic dermatitis, diabetes, and leukemia, its prophylactic value to food allergy remains to be proved.18,24
Nonetheless, parental lifestyle appeared to significantly impact the development of FHR. Smoking and alcohol drinking during pregnancy were clearly identified as risk factors. Exposure of children to parental smoking has been previously connected with allergic sensitization to airborne allergens, while there is still lack of clear significant evidence in the development of food allergy.25 We have identified the effect of maternal smoking during pregnancy or during infancy as a significant risk factor for FA+ children, but the medical literature still debates on this, with some references mentioning it even as a protective factor.26 Furthermore, alcohol consumption by pregnant mothers appeared significant, but the possible etiologic connection is unknown, and these outcomes should be further assessed in the future.
Furthermore, a parent being occupied in a profession related to the food development, production, processing or distribution, as well as the use of latex gloves at work, were significantly correlated to the development of food allergy in their offspring. Of course, obvious immunological connection cannot be decided, but more research could reveal the mechanisms related to this outcome.
Moreover, a trend for a protective effect in children who visited the kitchen area during cooking was accounted, without a statistical significance though. Again, this could be a valuable knowledge for further investigation.
The hygiene hypothesis has described the increased susceptibility to atopy due to limited early childhood exposure to infectious agents, with a diverged immune system development. However, data regarding the relation of the hygiene hypothesis with food allergy are contradictory.27 Our finding that most FA+ children were family’s first born might support the hygiene hypothesis, since first-born infants are not exposed to germ contagions by siblings. On the contrary, the fact that most of our FA+ children had followed day nursery, were sharing room with their siblings, or used antibiotics with the same frequency as healthy children, are opposing to a connection of food allergy to the hygiene hypothesis.28
A major drawback of our study was the low response rate (6.7%), resulting in a low number of participants with confirmed food allergy. However, this could be a result of the low rates of or the limited knowledge of food allergy in Cyprus. As shown elsewhere not being familiar with a disease limits one’s interest in providing information or participating in studies related to the disease.29
Our study for the first time provides important information about the profile of food allergic children in Cyprus and significant correlations with risk factors that can become the springboard for further studies related to food allergy and food sensitization.
REFERENCES
1. Sicherer SH, Sampson HA. Food allergy: A review and update on epidemiology, pathogenesis, diagnosis, prevention, and management. J Allergy Clin Immunol. 2018;141:41–58. 10.1016/j.jaci.2017.11.003
2. Savage J, Johns CB. Food allergy: Epidemiology and natural history. Immunol Allergy Clin North Am. 2015;35:45–59. 10.1016/j.iac.2014.09.004
3. Nwaru BI, Hickstein L, Panesar SS, Muraro A, Werfel T, Cardona V, et al. The epidemiology of food allergy in Europe: A systematic review and meta-analysis. Allergy. 2014;69:62–75. 10.1111/all.12305
4. Cochrane S, Beyer K, Clausen M, Wjst M, Hiller R, Nicoletti C, et al. Factors influencing the incidence and prevalence of food allergy. Allergy. 2009;64:1246–55. 10.1111/j.1398-9995.2009.02128.x
5. Bartra J, García-Moral A, Enrique E. Geographical differences in food allergy. Bundesgesundheitsblatt Gesundheitsforsch Gesundheitsschutz. 2016;59:755–763. 10.1007/s00103-016-2357-0
6. Burks AW, Tang M, Sicherer S, Muraro A, Eigenmann PA, Ebisawa M, et al. ICON: Food allergy. J Allergy Clin Immunol. 2012;129:906–920. 10.1016/j.jaci.2012.02.001
7. Alexandre-Silva GM, Brito-Souza PA, Oliveira ACS, Cerni FA, Zottich U, Pucca MB. The hygiene hypothesis at a glance: Early exposures, immune mechanism and novel therapies. Acta Trop. 2018;188:16–26. 10.1016/j.actatropica.2018.08.032
8. Sicherer SH, Sampson HA. Food allergy: Epidemiology, pathogenesis, diagnosis, and treatment. J Allergy Clin Immunol. 2014;133:291–307. 10.1016/j.jaci.2013.11.020
9. Roehr CC, Edenharter G, Reimann S, Ehlers I, Worm M, Zuberbier T, et al. Food allergy and non-allergic food hypersensitivity in children and adolescents. Clin Exp Allergy. 2004;34:1534–41. 10.1111/j.1365-2222.2004.02080.x
10. Noimark L, Cox HE. Nutritional problems related to food allergy in childhood. Pediatr Allergy Immunol. 2008;19:188–195. 10.1111/j.1399-3038.2007.00700.x
11. Wassenberg J, Cochard MM, DunnGalvin A, Ballabeni P, Flokstra-de Blok BMJ, Newman CJ, et al. Parent perceived quality of life is age-dependent in children with food allergy. Pediatr Allergy Immunol. 2012;23:412–419. 10.1111/j.1399-3038.2012.01310.x
12. Kavaliûnas A, Surkiene G, Dubakiene R, Zagminas K, Stukas R. Potential risk factors of food allergy in children: EuroPrevall project results in Vilnius, Lithuania. Health. 2013;5:2032–8. 10.4236/health.2013.512275
13. Kummeling I, Mills ENC, Clausen M, Dubakiene R, Frarnãndez Pérez C, Fernández-Rivas M, et al. The EuroPrevall surveys on the prevalence of food allergies in children and adults: Background and study methodology. Allergy. 2009;64:1493–97. 10.1111/j.1398-9995.2009.02046.x
14. Vassilopoulou E, Christoforou C, Andreou E, Heraclides A. Effects of food allergy on the dietary habits and intake of primary schools’ cypriot children. Eur Ann Allergy Clin Immunol. 2017;49:181–185. 10.23822/EurAnnACI.1764-1489.07
15. Templeton GF. A two-step approach for transforming continuous variables to normal: Implications and recommendations for IS research. Commun Assoc Inform Syst. 2011;28. 10.17705/1CAIS.02804
16. Legendre P, Legendre L. Numerical Ecology. 2nd ed. Elsevier; Amsterdam,1998.
17. Muraro A, Halken S, Arshad SH, Beyer K, Dubois AEJ, Du Toit G, et al. EAACI food allergy and anaphylaxis Guidelines. Primary prevention of food allergy. Allergy. 2014;69:590–601. 10.1111/all.12398
18. Grimshaw KEC, Allen K, Edwards CA, Beyer K, Boulay A, Van Der Aa LB, et al. Infant feeding and allergy prevention: A review of current knowledge and recommendations. A EuroPrevall state of the art paper. Allergy. 2009;64: 1407–16. 10.1111/j.1398-9995.2009.02172.x
19. Rigal N, Reiter F, Morice C, De Boissieu D, Dupont C. Impact du régime d’éviction sur la néophobie dans le cadre d’une allergie alimentaire chez l’enfant: Étude exploratoire. Arch Pediatr. 2005;12:1714–720. 10.1016/j.arcped.2005.02.031
20. Dovey TM, Staples PA, Gibson EL, Halford JCG. Food neophobia and “picky/fussy” eating in children: A review. Appetite. 2008;50:181–193. 10.1016/j.appet.2007.09.009
21. Kutbi HA, Alhatmi AA, Alsulami MH, Alghamdi SS, Albagar SM, Mumena WA et al. Food neophobia and pickiness among children and associations with socioenvironmental and cognitive factors. Appetite. 2019;142:104373. 10.1016/j.appet.2019.104373
22. Amoli MM, Hand S, Hajeer AH, Jones KP, Rolf S, Sting C, et al. Polymorphism in the STAT6 gene encodes risk for nut allergy. Genes Immun. 2002;3:220–224. 10.1038/sj.gene.6363872
23. Hand S, Darke C, Thompson J, Stingl C, Rolf S, Jones KP, et al. Human leucocyte antigen polymorphisms in nut-allergic patients in South Wales. Clin Exp Allergy. 2004;34:720–724. 10.1111/j.1365-2222.2004.1932.x
24. Goldsmith AJ, Koplin JJ, Lowe AJ, Tang MLK, Matheson MC, Robinson M, et al. Formula and breast feeding in infant food allergy: A population-based study. J Paediatr Child Health. 2016;52:377–384. 10.1111/jpc.13109
25. Raherison C, Pénard-Morand C, Moreau D, Caillaud D, Charpin D, Kopferschmitt C, et al. Smoking exposure and allergic sensitization in children according to maternal allergies. Ann Allergy Asthma Immunol. 2008;100:351–357. 10.1016/S1081-1206(10)60598-4
26. Hjern A, Hedberg A, Haglund B, Rosén M. Does tobacco smoke prevent atopic disorders? A study of two generations of Swedish residents. Clin Exp Allergy. 2001;31:908–914. 10.1046/j.1365-2222.2001.01096.x
27. Lack G. Update on risk factors for food allergy. J Allergy Clin Immunol. 2012;129:1187–97. 10.1016/j.jaci.2012.02.036
28. Hirsch AG, Pollak J, Glass TA, Poulsen MN, Baily-Davis L, Mowery J, et al. Early-life antibiotic use and subsequent diagnosis of food allergy and allergic diseases. Clin Exp Allergy. 2017;47:236–244. 10.1111/cea.12807
29. Grady C. Payment of clinical research subjects. J Clin Invest. 2005;115:1681–87. 10.1172/JCI25694