
Download
REVIEW ARTICLE
From bench to bedside: advances in standardized oral immunotherapy and early predictors of persistent cow’s milk allergy in children
Asena Pinar Sefera,b,c, Elif Karakoc-Aydinerb,c,d,e,f*
aDivision of Allergy and Immunology, Department of Pediatrics, School of Medicine, Recep Tayyip Erdogan University, Rize, Türkiye
bIsil Berat Barlan Center for Translational Medicine, Istanbul, Türkiye
cImmune Deficiency Research and Application Center, Istanbul, Türkiye
dDivision of Allergy and Immunology, Department of Pediatrics, Faculty of Medicine, Marmara University, Istanbul, Türkiye
eIstanbul Jeffrey Modell Diagnostic Center for Primary Immunodeficiency Diseases, Istanbul, Türkiye
fEuropean Academy of Allergy and Clinical Immunology, Marmara University Hospital Center of Excellence, Istanbul, Türkiye
Abstract
Immunoglobulin E (IgE)-mediated cow’s milk allergy (CMA) remains the most prevalent pediatric food allergy and a major cause of early-life anaphylaxis, with a substantial proportion of children developing persistent disease despite traditional avoidance-based management. Oral immunotherapy (OIT) has emerged as a proactive strategy that modulates the allergic immune response through controlled and sustained allergen exposure, shifting immunity from T-helper (Th) 2-dominant pathways toward a more regulatory and tolerogenic profile. Current evidence from randomized trials and real-world cohorts demonstrates that cow’s milk oral immunotherapy (CM-OIT) achieves desensitization in most treated children, reduces accidental reaction risk, and improves quality of life, although sustained unresponsiveness remains variable and protocol-dependent. Marked heterogeneity exists across protocols regarding dosing, antigen formulation, maintenance targets, and escalation speed, reflecting differing therapeutic philosophies rather than standardized practice. Safety concerns, including dose-related reactions and rare cases of eosinophilic esophagitis, underscore the need for careful patient selection, optimization of comorbid atopic diseases, and shared decision-making. Advances in precision immunology, including component-resolved diagnostics, epitope mapping, basophil activation testing, and emerging transcriptomic and microbiome signatures, now enable the earlier identification of children at high risk of persistent CMA who may benefit most from OIT, while low-risk phenotypes can be safely observed. Adjunctive biologic therapy, particularly anti-IgE agents, has improved tolerability and expanded eligibility in high-risk patients. This review synthesizes current evidence on efficacy, safety, biomarkers, protocols, and adjunctive strategies, emphasizing a personalized, risk-adapted approach to CM-OIT and outlining future directions toward standardized formulations, biomarker-guided stratification, and integrated biologic-assisted immunomodulation.
Key words: cow’s milk allergy, oral immunotherapy, pediatric food allergy, predictive markers, risk stratification
*Corresponding author: Elif Karakoc-Aydiner, Marmara University, Division of Pediatric Allergy/Immunology, Fevzi Çakmak Mah. No: 41, Pendik /Istanbul/Türkiye. Email address: [email protected]
Received 20 November 2025; Accepted 18 February 2026; Available online 10 April 2026
DOI: 10.15586/aei.v54isp1.1638
Copyright: Sefer AP and Aydiner EK
License: This open access article is licensed under Creative Commons Attribution 4.0 International (CC BY 4.0). http://creativecommons.org/licenses/by/4.0/
Introduction
Immunoglobulin E (IgE)-mediated cow’s milk allergy (CMA) remains the most common pediatric food allergy worldwide, affecting approximately 2–3% of children. Although many patients present with mild to moderate cutaneous or gastrointestinal symptoms, CMA has remained a leading cause of food-induced anaphylaxis in early life, accounting for up to 10–20% of anaphylactic reactions in infants and young children. Fatal reactions to cow’s milk are rare but have been reported, particularly in children with concomitant asthma or delayed recognition of symptoms. Among milk proteins, casein and whey proteins, especially β-lactoglobulin and α-lactalbumin, are the major allergens, with casein sensitization being associated with more persistent and severe disease. Cow’s milk remains one of the most prevalent and clinically significant food allergens worldwide.1–5 Although up to 50–90% of affected children eventually surmount CMA, a substantial subset develops a persistent and clinically impactful disease course extending into later childhood or adolescence.6,7 For these children, strict dietary avoidance has traditionally been the cornerstone of management. However, this passive strategy does not modulate underlying immune reactivity, places a lifelong psychosocial and nutritional burden on families, and fails to prevent accidental reactions despite optimal education and emergency preparedness.8–10
Oral immunotherapy (OIT) has been increasingly explored as a disease-modifying approach for the management of food allergy. Previous studies have demonstrated the efficacy of OIT protocols in inducing desensitization in common food allergies, including peanut, hen’s egg, and tree nuts, leading to reduced reaction severity and improved quality of life (QoL) in selected patients. These experiences have provided a foundation for investigating OIT strategies in CMA.11 Cow’s milk oral immunotherapy (CM-OIT) aims to raise the reactivity threshold (desensitization) and, in some cases, achieve sustained unresponsiveness (SU), which is a lasting tolerance after stopping treatment. Pilot studies have advanced to randomized controlled trials (RCT) and real-world cohort data, leading to growing international recognition of CM-OIT as a viable treatment option for carefully selected children. Several national guidelines now recognize CM-OIT for persistent IgE-mediated CMA. However, protocols remain highly heterogeneous, and there is no universally standardized regimen.12–16 Meanwhile, advances in precision immunology, including component-resolved diagnostics, basophil activation testing (BAT), serum allergen-specific immunoglobulin E (sIgE)/epitope profiling, and evolving transcriptomic and microbiome signatures, now enable the identification of children at high risk of persistent CMA before irreversible T-helper (Th) 2 immune memory is established.17,18
This review synthesizes current clinical evidence on CM-OIT, exploring its immunologic basis, treatment efficacy, safety profile, patient selection criteria, and the emerging significance of biomarkers and biologic adjuncts. Instead of advocating a one-size-fits-all protocol, it emphasizes a risk- and goal-based approach that tailors OIT intensity to each individual’s immunologic and clinical profiles.
Immunopathogenesis
Immunoglobulin E-mediated CMA results from a failure of early-life oral tolerance, driven by impaired epithelial barrier integrity, altered antigen presentation, and skewed T-cell differentiation.7 Upon exposure to cow’s milk proteins, most notably caseins and whey proteins such as β-lactoglobulin and α-lactalbumin, antigen-presenting cells in the gut mucosa present these allergens to naïve cluster of differentiation 4+ (CD4+) T cells. Instead of differentiating into regulatory T cells (Tregs), these cells aberrantly polarize toward a Th2 phenotype under the influence of cytokines, such as interleukin (IL)-4, IL-5, and IL-13. This Th2-skewed response promotes class switching to allergen-specific IgE, which binds to high-affinity FcεRI (high-affinity IgE) receptors on mast cells and basophils. Upon re-exposure, even trace amounts of cow’s milk allergens can cross-link IgE and trigger immediate hypersensitivity reactions through rapid release of histamine and other inflammatory mediators.19
In children who fail to outgrow CMA, this allergic immune profile is reinforced immunologically. Persistent disease is characterized by the expansion of long-lived Th2 memory cells, insufficient induction of suppressive FoxP3+ Tregs, low levels of protective IgG4 (constitutes about 5% of total immunoglobulin G [IgG]) “blocking antibodies,” and, in some cases, spreading of progressive epitope. Additionally, gut dysbiosis and epithelial alarmin signaling, particularly Interleukin-33 (IL-33) and thymic stromal lymphopoietin (TSLP), perpetuate Th2 activation and impair tolerance acquisition, creating a self-sustaining allergic loop.20
Oral immunotherapy is designed to counteract this pathogenic cascade by actively reprogramming the immune system rather than suppressing exposure. Through gradual, controlled allergen administration, OIT progressively increases the activation thresholds of mast cells and basophils (early desensitization) while shifting humoral immunity toward a more protective profile characterized by rising allergen-specific IgG4 and eventual decline in IgE. Importantly, OIT promotes the expansion of IL-10- and transforming growth factor-beta (TGF-β)-producing Tregs, along with a relative increase in interferon gamma (IFN-γ)-secreting Th1 cells, thereby correcting the Th2-dominant imbalance.21,22 Over time, this adaptive remodeling may extend beyond transient protection and enable SU, although this outcome remains variable and patient-dependent.
Clinical Efficacy of Cow’s Milk Oral Immunotherapy
Desensitization is the most reliably proven and clinically significant outcome of CM-OIT, offering meaningful protection against accidental ingestion and cross-contamination, benefits that significantly reduce caregiver anxiety and daily disease burden.23
In various RCTs, approximately 60–70% of children with IgE-mediated CMA achieve clinically meaningful desensitization, supported by meta-analyses reporting pooled success proportion of around 68%.24–29 Cochrane evidence also confirms tolerance to 150–243 mL of milk in 62% of treated children, compared to only 8% in elimination-only controls.30 Two recent high-quality meta-analyses further confirmed these findings, showing a relative risk of 2.51 (95% Confidence Interval [CI] 1.54–4.09) with a significant increase in tolerated threshold (standardized mean difference [SMD] ~3.6), and an even larger effect size in another review (relative risk [RR]: 5.88; 95% CI 2.27–15.18), representing one of the most notable therapeutic impacts observed to date in food allergy immunotherapy.12,15
These clinical effects are supported by consistent immunologic evidence. Several independent studies show significant decrease in milk- and casein-specific IgE, along with a notable increase in milk-specific IgG4, indicating a favorable shift toward a blocking antibody-dominated immune profile.26,27,31,32 Although cytokine and cellular immune data remain limited across studies, the steady decline in effector activity and increase in regulatory signals strongly suggest genuine immune modulation, rather than just temporary suppression of reactivity.15,21
While desensitization indicates an active, treatment-dependent state, SU represents a more durable and clinically meaningful outcome. Conceptually, SU reflects treatment-independent immune regulation and is therefore considered a closer indicator of genuine immunologic tolerance. However, its assessment remains far from standardized processing. Current CM-OIT trials define SU after withdrawal periods ranging from 2 weeks to 6 months, creating significant variability across studies and complicating inter-study comparisons.33,34 Early observational studies showed promising persistence; long-term follow-up reveals that about 46–65% of patients who initially achieved desensitization can still regularly consume cow’s milk after 4–7 years.35–37 RCTs report SU in about 30–60% of patients after 1–3 years of OIT, although long-term durability appears considerably lower in real-world.25,38 Together, these findings emphasize a critical distinction: CM-OIT can induce SU in a significant group of patients, but lifelong, exposure-independent tolerance remains unpredictable and unproven in most cases. SU should therefore be regarded not as a definitive cure but as a favorable immunologic trend, one that might still require continued, or at least regular, allergen exposure to persist.
Quality of Life Outcomes
While desensitization remains the primary clinical endpoint of CM-OIT, its effect on health-related QoL has been relatively underinvestigated. Dantzer et al. have used a validated disease-specific instrument to evaluate QoL, utilizing the Food Allergy Quality of Life Parent Form (FAQLQ-PF) or Food Allergy Quality of Life Child Form (FAQLQ-CF). Notably, a clinically meaningful improvement was observed from baseline to 12 months of treatment.39 Another study involving 191 children aged 4–12 years undergoing OIT for cow’s milk and other food allergies (including egg, peanut, sesame, or tree nuts) demonstrated that FAQLQ-PF significantly improved from the initiation to the maintenance phase of OIT across multiple domains. In contrast, scores remained stable in the control group. Factors associated with greater improvement included having a single food allergy, younger age at initiation of OIT, and a poorer baseline QoL score.40 Although limited in number, these findings are consistent with real-world observations that successful desensitization lowers anticipatory anxiety, enhances participation in social and school activities, and reduces the psychologic burden predominantly experienced by caregivers.
These data highlight the importance of including QoL as a co-primary endpoint in future CM-OIT trials, particularly given that risk perception and emotional safety often influence family decisions more than biochemical or immunologic results. Incorporating standardized, validated QoL tools should be considered essential for accurately measuring the real-world therapeutic benefits of OIT beyond immune desensitization alone.
Protocols and Optimization Strategies for Cow’s Milk Oral Immunotherapy
An internationally standardized protocol for CM-OIT has yet to be established. Current clinical practice remains highly heterogeneous regarding the optimal form of milk protein, initial and maintenance doses, and treatment duration, shaped more by differing therapeutic philosophies than by technical limitations.14,16,41,42 Some protocols aim for complete dietary liberalization, while others focus on minimizing risk and preventing accidental exposure, rather than allowing unrestricted intake. Despite this variability, most CM-OIT programs follow a standard three-phase structure: an initial dose escalation (IDE) performed under medical supervision to determine an individualized safe starting dose; a build-up phase with stepwise outpatient dosing every 1–2 weeks and daily home administration; and a maintenance phase, which may continue for months to years to preserve desensitization and, in selected cases, attempt progression toward SU.34,43
Globally, rush or semi-rush escalation models target rapid dose achievement, sometimes reaching maintenance within days through aggressive intra-hospital up-dosing.44 In contrast, traditional slow-updosing strategies increase doses more gradually over weeks to months, emphasizing safety and tolerability at the cost of delayed protection.45 A similar divergence occurs in maintenance targets: high-dose protocols aim for 100–200 mL/day to achieve full dietary normalization, whereas low-dose protocols (3–10 mL/day) focus on offering strong protection against accidental exposures while minimizing burdens and adverse events (Table 1).44,46,47
Table 1 Comparison of cow’s milk oral ımmunotherapy protocols.
| Protocol | IDE duration | Build-up speed | Maintenance dose | Overall duration | Advantages | Disadvantages | Ideal patient profile |
|---|---|---|---|---|---|---|---|
| Slow OIT41,61 | 1–2 h, low initial dose | Dose increased every 1–2 weeks | 50–200 mL/day1 | 6–12+ months | Lower reaction rate; gradual adaptation; high family acceptability | Long duration; delayed protection | Moderate-risk CMA; controlled asthma; families preferring stepwise progression |
| Rush OIT29,44,47 | 1–2 Days; rapid multi-step | Multiple rapid increase on the same day | 100–200 mL/day2 | 3–7 Days to maintenance | Very rapid desensitization; early high protection | High rate of mild–moderate reactions; increased anaphylaxis risk, requires experienced center | Low–moderate risk; highly motivated families; hospital-monitored setting |
| Semi-rush OIT34,43 | Single-day abbreviated IDE | Daily or alternate-day increases | 100–200 mL/day2 | 1–3 months | Faster than slow OIT; safer than full rush | Moderate reaction risk | Moderate-risk children; centers balancing speed and safety |
| LOIT46,52,53 | 1–2 h | Slow, conservative up-dosing | 3–10 mL/day3 |
6–24 months | Very safe; lowest epinephrine use; strong adherence; low dropout rate | Full dietary liberalization less likely; slower IgE decline | High-risk CMA (high IgE, anaphylaxis history, asthma/AD); families prioritizing safety |
| HOIT25,44,47,54 | Standard IDE (1–2 h) |
Weekly or semi-weekly increases | 100–200 mL/day2 | 3–6 months | Higher likelihood of complete liberalization; stronger immunologic remodeling | More adverse reactions; increased dropout, higher EoE risk | Low- or moderate-risk patients aiming for full unrestricted milk intake |
Notes:1High-dose maintenance (50–200 mL/day) is typically used in protocols aiming for full dietary liberalization and robust long-term desensitization.
2Maintenance doses of 100–200 mL/day represent conventional high-dose strategies designed to normalize milk intake; accelerated protocols reach this threshold earlier.
3Low-dose maintenance (3–10 mL/day; ~7–170 mg protein) provides strong protection against accidental exposure with significantly fewer adverse events, suitable for high-risk patients. CMA: cow’s milk allergy; OIT: oral immunotherapy; IDE: initial dose escalation; LOIT: low-dose oral immunotherapy; HOIT: high-dose oral immunotherapy; EoE: eosinophilic esophagitis; AD: atopic dermatitis.
Antigen formulation remains a key challenge for clinical translation. Cow’s milk contains both heat-sensitive whey proteins and heat-stable caseins, making its immunogenicity highly dependent on processing temperature, duration, and the matrix composition. Raw or minimally processed milk preserves conformational epitopes, leading to strong IgE cross-linking and, in some trials, better desensitization efficacy compared to heated formulations.48 Extensively heated or baked milk destroys conformational epitopes but preserves linear casein epitopes, providing a less inflammatory option, especially suitable for highly sensitized or anaphylaxis-prone children. However, household-baked products (such as muffins and pancakes) exhibit uncontrolled variability in protein distribution, heat penetration, and epitope preservation, issues that directly reduce reproducibility and lead to conflicting trial outcomes. In response, pharmaceutically engineered and analytical validation platforms, such as the SUTMEK (Standardized Bakery Product/Standardize Edilmiş Fırın Ürünü) (Turkey) and the Japanese Heated Milk Powder systems, have emerged, offering standardized thermal processing, accurate protein measurement, preserved epitope integrity, matched placebos, and suitability for Double-Blind Placebo-Controlled Food Challenges (DBPCFC) and therapeutic OIT at a regulatory level.49,50 Early feasibility studies have shown promising translational signals, with approximately 60% of participants achieving baked-milk tolerance and successfully incorporating heated milk into their daily intake.
Standardization of antigen formulations, along with harmonizing dosing thresholds, maintenance strategy definitions, and immunologic endpoints, is now an urgent requirement for moving CM-OIT from heterogeneous practices to truly global precision immunotherapy.
Safety Profile of Cow’s Milk Oral Immunotherapy
Safety remains a key concern in OIT, with adverse reactions most common during the initial escalation and build-up phases. Although most reactions are mild and self-limited, severe anaphylaxis can still occur.25 Notably, CMA carries a higher intrinsic risk than other allergens; adrenaline is administered in approximately 26.8% of milk OIT cases, compared with 11.3% for non-milk allergens.29 In a 20-year retrospective study comprising 342 children with persistent CMA, 3.5% experienced severe reactions during therapy, and 6.3% of those who discontinued OIT suffered severe reactions following accidental milk ingestion, including two fatalities.51 These results highlight that although OIT shifts the timing and setting of allergic reactions to a supervised environment, it does not eliminate the risk. Notably, meta-analytic data suggest that OIT does not significantly increase the overall proportion of adverse reactions compared with control groups (RR: 2.05; 95% CI 0.96–4.37), nor the proportion of severe reactions (RR: 2.65; 95% CI 0.79–16.90), but it highlights substantial heterogeneity across protocols. A minority of patients (about 4%) may develop eosinophilic esophagitis (EoE), a late-onset complication that requires prolonged monitoring of maintenance.15
Given that traditional high-dose oral immunotherapy (HOIT) protocols have been associated with long-term reactions in up to 75% of patients and anaphylaxis in approximately 19%, there has been a progressive shift toward safer, risk-adapted approaches, such as low-dose oral immunotherapy (LOIT) (Table 1).47 Controlled trials using daily maintenance doses as low as 0.2–5 mL (7–170 mg protein) have achieved SU in 33–38% of children, with markedly lower adrenaline use (0–8%).46,52 Long-term follow-up reveals higher adherence and lower dropout proportions with LOIT (11% vs. 24% in HOIT), accompanied by meaningful immunologic remodeling, including a 78% reduction in milk-specific IgE (although slightly less pronounced than the 88% reduction observed with HOIT).53,54 Moreover, reducing the allergenicity of the allergen, for example, by using heated or baked milk, has been shown to improve tolerability without compromising immunologic benefit. In one study conducted by Nagakura et al., SU proportions were comparable between heated and raw milk OIT (35% vs. 50%), yet the heated group experienced fewer adverse reactions.49
Collectively, these data support an evolving paradigm toward personalized, precision-based OIT strategies that prioritize safety without sacrificing efficacy, incorporating lower maintenance doses, structurally modified antigen formulations, and, where appropriate, adjunctive biologic therapies in high-risk patients.
Patient Selection and Indications for Cow’s Milk Oral Immunotherapy
Cow’s milk OIT has now been included in international guidelines as a treatment option for children with IgE-mediated CMA. It is a potential therapeutic option, particularly when strict avoidance therapy is ineffective, imposes significant dietary or psychosocial limitations, or significantly impacts QoL. A confirmed diagnosis is crucial before starting OIT. In the absence of a clear history of immediate hypersensitivity to cow’s milk or dairy product, an oral food challenge (OFC) must be performed to confirm the diagnosis and establish a baseline reactivity threshold, which serves as an individualized reference for monitoring treatment.14,16,41
Given the highly heterogeneous immunologic and clinical profiles observed in CMA, it is now widely accepted that no single OIT protocol can be applied universally to all patients. Most international guidelines recommend prioritizing OIT for children aged ≥4 years because most low-risk children spontaneously outgrow the allergy by age 5, and early intervention may unnecessarily increase treatment burden during this natural tolerance window.14 However, recent studies have suggested a potential advantage for earlier intervention in carefully selected high-risk patients, particularly those with high baseline casein-specific IgE, atopic multimorbidity, or a history of prior anaphylaxis, in whom spontaneous resolution is doubtful.55,56 Beyond persistence prediction, baseline immunologic burden and reaction phenotype now play a central role in therapeutic decision-making. Parameters such as milk- or casein-specific IgE levels, Skin Prick Test (SPT) wheal diameter, basophil activation thresholds, and atopic multimorbidity (e.g., asthma and AD) are increasingly used not only to predict OIT responsiveness but also to anticipate safety in the escalation phase.34,57 Consequently, high-risk patients (e.g., those with very high sIgE, a history of anaphylaxis, or uncontrolled asthma) are now preferentially directed toward low-dose, heated/baked antigen protocols or biologic-assisted induction. In contrast, moderate-risk children with persistent CMA for ≥4 years represent ideal candidates for standard-dose conventional or semi-rush OIT.47,58 Several baked-milk or low-dose protocols have reported high tolerance proportions within 24–36 months, but with simultaneously high reaction proportions, emphasizing the need for precision in-patient selection rather than universal early treatment.59
Because CM-OIT is a long-duration, adherence-dependent procedure associated with a predictable risk of adverse reactions, careful assessment of family readiness is critical.60 This includes assessing motivation, reliability, and the ability to recognize and manage reactions promptly. Families with high anxiety, poor access to emergency care, or difficulty in attending frequent clinic visits may be better suited for low-dose or stepwise OIT, or even delayed OIT with interim introduction of baked-milk.61
Before starting treatment, uncontrolled asthma and moderate-to-severe atopic dermatitis (AD) should be medically optimized, as these conditions significantly raise the risk of severe reactions. Additional relative contraindications include mastocytosis, active malignancy, systemic autoimmune disease, or any condition that prevents safe adrenaline use. A history of anaphylaxis to cow’s milk is not usually an absolute contraindication in most expert-led programs as long as the family is fully trained and therapy is provided in an experienced and well-equipped center.14,34
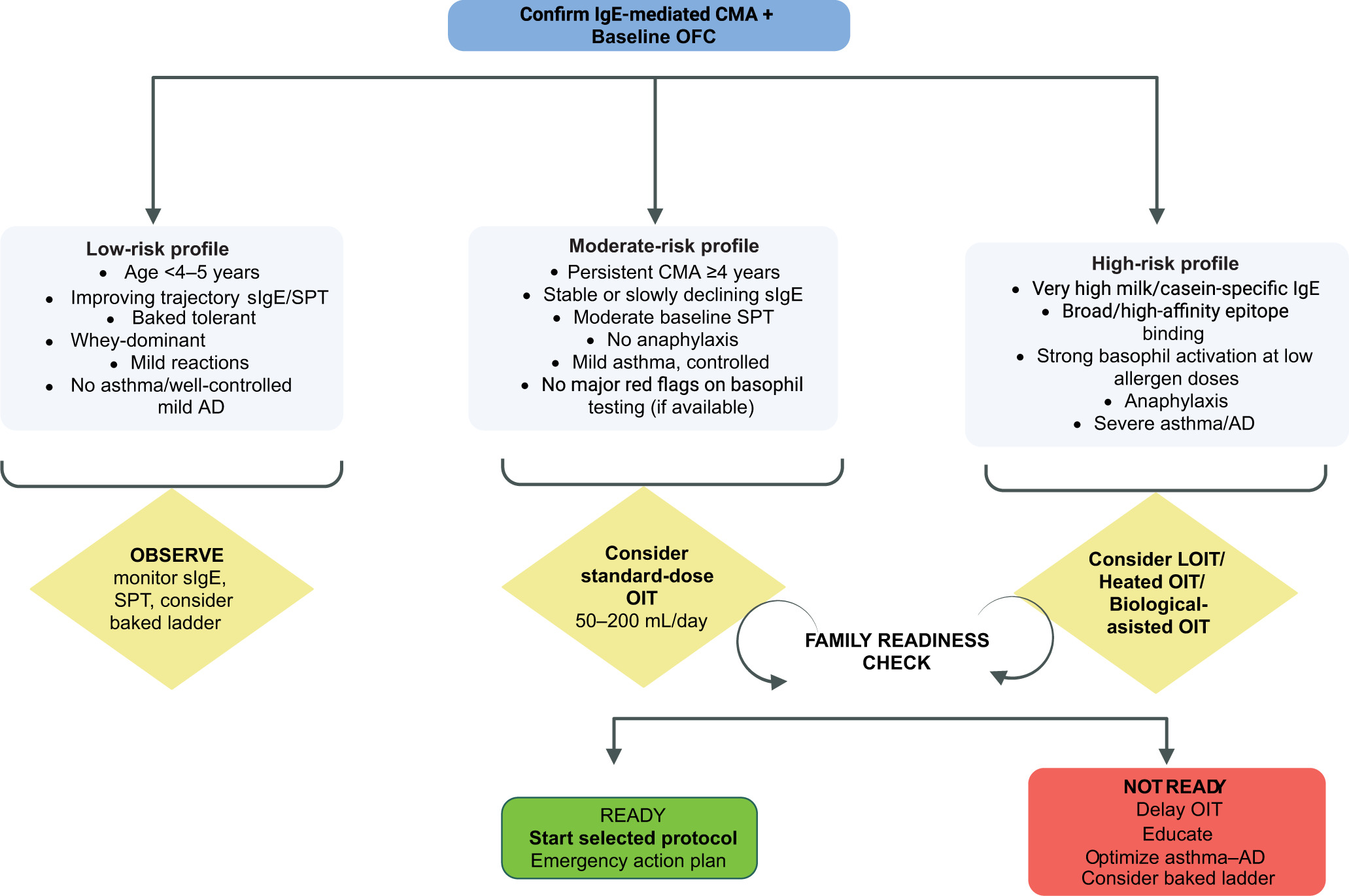
A risk-stratified patient selection algorithm for CM-OIT is presented in Figure 1.
Figure 1 Risk-stratified clinical algorithm for ınitiating cow’s milk oral ımmunotherapy (CM-OIT). The figure illustrates a stepwise, risk-adapted decision algorithm integrating clinical, immunologic, and family-centered factors before initiating oral immunotherapy in children with IgE-mediated cow’s milk allergy. Notes. AD: atopic dermatitis; CMA: cow’s milk allergy; LOIT: low-dose oral immunotherapy; OFC: oral food challenge; OIT: oral immunotherapy; sIgE: serum allergen-specific IgE; SPT: skin prick test.
Predictive Biomarkers for Treatment Selection Prior to Cow’s Milk Oral Immunotherapy
Emerging data support a biomarker-guided approach to determining who should start OIT versus who does not need to.62 Children with low and declining milk/casein sIgE trajectories, shrinking SPT wheals, limited epitope breadth (narrow IgE recognition, predominantly whey, rather than casein), and a lower IgE–IgG4 ratio tend to follow a spontaneous tolerance path and may be observed rather than treated.18 Recent infant cohort studies further support this, showing that the absence of anaphylaxis at initial presentation, no family history of atopy, and low baseline milk-/casein-specific IgE levels independently predict early tolerance to baked forms within the first 2 years of life.7,18 By contrast, high and persistent casein-specific sIgE, broad/high-affinity IgE epitope repertoires (including casein/Bos d 8 [casein] binding), robust basophil activation at low allergen doses (low EC50; strong CD63/CD203c response), and rising or plateaued sIgE over time signal immunologic persistence and favor early OIT consideration.7,29,62–64 Clinical context refines these signals: multimorbidity (uncontrolled asthma, severe AD), history of anaphylaxis, and older age with ongoing reactivity (≥4–5 years) increase the pretest probability of persistence, whereas infants/toddlers with minimal SPT, low sIgE, and improving trajectories often achieve tolerance with observation alone.2,65,66 Exploratory markers (e.g., component-resolved diagnostics, serum/secretory IgA, blood transcriptomic Th2/Treg signatures, and microbiome features) are increasingly promising but require further standardization and external validation.15,34 Practically, a composite, longitudinal algorithm that integrates sIgE/SPT kinetics, cysteine-rich domains (CRD)-defined epitope dominance, and BAT thresholds, layered on clinical risk, is likely to outperform any single marker in selecting candidates for early, benefit-weighted CM-OIT.
Adjunctive Strategies
Despite growing success with CM-OIT, variability in long-term durability and concerns about safety have accelerated interest in adjunctive strategies designed to enhance tolerability, accelerate dose progression, or deepen immune deviation. Among these, biologic agents have emerged as the most promising co-therapeutic option, especially in patients with high baseline IgE, severe atopic multimorbidity, or poor protocol tolerance.58,67
Omalizumab (anti-IgE), recently approved by FDA for food allergy, is the most extensively studied adjunct to CM-OIT.68 Multiple randomized trials demonstrate that pre-treatment with omalizumab substantially reduces escalation-phase reactions and enables faster progression to maintenance, particularly in children with high milk-specific IgE or a history of anaphylaxis. However, while omalizumab clearly improves safety and tolerability, its effect on SU remains inconsistent.69,70
Other biologics, such as dupilumab (anti-interleukin-4 receptor alpha [IL-4Rα]) and etokimab (anti-IL-33), target upstream Th2 signaling and may offer dual advantages, not only reducing reactivity risk but also potentially enhancing genuine immune deviation during OIT. Early-phase studies in cow’s milk and peanut OIT show encouraging trends toward deeper modulatory effects.34,47,48
Future Perspectives
The therapeutic landscape of IgE-mediated CMA is now shifting from empiric desensitization toward precision-guided immune modulation, driven by three major forces actively reshaping the field: protocol standardization, immunologic stratification, and the integration of biologic adjuncts. The most immediate need remains the development and regulatory validation of standardized, pharmaceutical-grade allergen formulations that ensure reproducible protein content, epitope integrity, and DBPCFC compatibility. This not only eliminates significant heterogeneity sources across current OIT studies but also enables global harmonization of clinical trial endpoints and safety thresholds. In parallel, early-stage patient stratification is expected to move rapidly from crude sIgE and SPT cutoffs to multidimensional biomarker algorithms incorporating component-resolved diagnostics, epitope diversity mapping, basophil reactivity, microbiome signatures, and eventually transcriptomic tolerance-predictive profiles. Such tools are on the verge of enabling truly risk-adaptive OIT, escalating aggressively only in low-risk immune phenotypes while guiding others toward low-dose, adjunct-assisted, or even non-OIT immune-repair strategies.
Perhaps the most transformative frontier is the emergence of biologic-adjunct OIT, where agents such as omalizumab or dupilumab are not merely used to “make OIT safer,” but also reimagined as immunologic gateways that unlock therapy in patients who were previously considered high-risk to attempt desensitization at all. Early data suggest that biologic-guided OIT could reduce escalation-phase morbidity, accelerate maintenance achievement, and expand therapeutic eligibility beyond the current “carefully selected” minority.
Conclusion
Cow’s milk allergy remains a common and potentially severe food allergy in childhood, with a substantial impact on patient safety, dietary practices, and family QoL. Our findings contribute to the growing body of evidence supporting OIT as a promising approach for selected children with CMA, offering the potential to increase reaction thresholds and reduce the risk of accidental reactions. Nevertheless, OIT should be implemented with careful patient selection, close monitoring, and appropriate expertise, given the risk of adverse reactions. Further prospective studies with standardized protocols and long-term follow-up are needed to better define the optimal candidates, safety profile, and sustained outcomes of OIT in CMA.
Mandatory Disclosure on Use of Artificial Intelligence
The authors declare that no AI-assisted tools were used in the preparation of this manuscript. All references have been manually verified for accuracy and relevance.
Author Contributions
Both authors contributed equally to this aritcle.
Conflicts of Interest
The authors declare no potential conflicts of interest with respect to research, authorship, and/or publication of this article.
Funding
None.
REFERENCES
1. Spolidoro GCI, Ali MM, Amera YT, Nyassi S, Lisik D, Ioannidou A, et al. Prevalence estimates of eight big food allergies in Europe: Updated systematic review and meta-analysis. Allergy. 2023;78(9):2361–417. 10.1111/all.15801
2. Schoemaker AA, Sprikkelman AB, Grimshaw KE, Roberts G, Grabenhenrich L, Rosenfeld L, et al. Incidence and natural history of challenge-proven cow’s milk allergy in European children--EuroPrevall birth cohort. Allergy. 2015;70(8):963–72. 10.1111/all.12630
3. Jarvinen KM, Sicherer SH, Sampson HA, Nowak-Wegrzyn A. Use of multiple doses of epinephrine in food-induced anaphylaxis in children. J Allergy Clin Immunol. 2008;122(1):133–8. 10.1016/j.jaci.2008.04.031
4. Aksoy AG, Boran P, Karakoc-Aydiner E, Gokcay G, Tamay ZU, Devecioglu E, et al. Prevalence of allergic disorders and risk factors associated with food allergy in Turkish preschoolers. Allergol Immunopathol (Madr). 2021;49(1):11–6. 10.15586/aei.v49i1.23
5. Perez-Codesido S, Grifol-Clar E, Petrone MB, Malumbres MG, Garban PA, Tejedor-Alonso MA. Frequency of fatal and recurrent anaphylaxis due to cow’s milk: A systematic review and meta-analysis of observational studies. Pediatr Allergy Immunol. 2023;34(7):e13977. 10.1111/pai.13977
6. Allen CW, Campbell DE, Kemp AS. Food allergy: Is strict avoidance the only answer? Pediatr Allergy Immunol. 2009;20(5):415–22. 10.1111/j.1399-3038.2008.00811.x
7. Wood RA, Sicherer SH, Vickery BP, Jones SM, Liu AH, Fleischer DM, et al. The natural history of milk allergy in an observational cohort. J Allergy Clin Immunol. 2013;131(3):805–12. 10.1016/j.jaci.2012.10.060
8. Sinai T, Goldberg MR, Nachshon L, Amitzur-Levy R, Yichie T, Katz Y, et al. Reduced final height and inadequate nutritional intake in cow’s milk-allergic young adults. J Allergy Clin Immunol Pract. 2019;7(2):509–15. 10.1016/j.jaip.2018.11.038
9. Engel ML, Warren CM, Herbert LJ, Pappalardo AA, Ramos A, Gupta RS. The psychosocial burden of pediatric food allergy in the United States: A population-based survey. J Allergy Clin Immunol Pract. 2025;13(3):630–8.e4. 10.1016/j.jaip.2024.12.007
10. Gunal O, Sefer AP, Utuk B, Altunbas MY, Güüngören EY, Babayeva R, Eltan SB, et al. Cross-sectional analysis of health quality, treatment satisfaction and adherence in children with food allergy. Clin Exp Health Sci. 2025;15:217–25. 10.33808/clinexphealthsci.1589757
11. McHenry M, Begin P, Chan ES, Latrous M, Kim H. Food oral immunotherapy. Allergy Asthma Clin Immunol. 2025;20(Suppl 3):82. 10.1186/s13223-025-00948-5
12. Riggioni C, Oton T, Carmona L, Du Toit G, Skypala I, Santos AF. Immunotherapy and biologics in the management of IgE-mediated food allergy: Systematic review and meta-analyses of efficacy and safety. Allergy. 2024;79(8):2097–127. 10.1111/all.16129
13. Bognanni A, Chu DK, Firmino RT, Arasi S, Waffenschmidt S, Agarwal A, et al. World Allergy Organization (WAO) Diagnosis and Rationale for Action against Cow’s Milk Allergy (DRACMA) Guideline Update–XIII–Oral immunotherapy for CMA–Systematic review. World Allergy Organ J. 2022;15(9):100682. 10.1016/j.waojou.2022.100682
14. Pajno GB, Fernandez-Rivas M, Arasi S, Roberts G, Akdis CA, Alvaro-Lozano M, et al. EAACI guidelines on allergen immunotherapy: IgE-mediated food allergy. Allergy. 2018;73(4):799–815. 10.1111/all.13319
15. Wang Y, Liu S, Lu M, Guo J, Lv C, Huang L. Oral immunotherapy for cow’s milk allergy in children: A systematic review and meta-analysis. Front Immunol. 2025;16:1570050. 10.3389/fimmu.2025.1570050
16. Begin P, Chan ES, Kim H, Wagner M, Cellier MS, Favron-Godbout C, et al. CSACI guidelines for the ethical, evidence-based and patient-oriented clinical practice of oral immunotherapy in IgE-mediated food allergy. Allergy Asthma Clin Immunol. 2020;16:20. 10.1186/s13223-020-0413-7
17. Esty B, Maciag MC, Bartnikas LM, Petty CR, MacGinnitie AJ, Sheehan WJ, et al. Predicting outcomes of baked egg and baked milk oral food challenges by using a ratio of food-specific IgE to total IgE. J Allergy Clin Immunol Pract. 2021;9(4):1750–2.e1. 10.1016/j.jaip.2020.11.004
18. Altunbas MY, Gungoren EY, Can S, Amirov R, Ozturk N, Bozkurt S, et al. Early markers of baked milk and egg tolerance in young children with IgE-mediated immediate reactions. Eur Ann Allergy Clin Immunol. 2026;58(2):86-96. 10.23822/EurAnnACI.1764-1489.383
19. Vitaliti G, Cimino C, Coco A, Pratico AD, Lionetti E. The immunopathogenesis of cow’s milk protein allergy (CMPA). Ital J Pediatr. 2012;38:35. 10.1186/1824-7288-38-35
20. Carnazza M, Werner R, Tiwari RK, Geliebter J, Li XM, Yang N. The etiology of IgE-mediated food allergy: Potential therapeutics and challenges. Int J Mol Sci. 2025;26(4). 10.3390/ijms26041563
21. Kulis MD, Patil SU, Wambre E, Vickery BP. Immune mechanisms of oral immunotherapy. J Allergy Clin Immunol. 2018;141(2):491–8. 10.1016/j.jaci.2017.12.979
22. Ramsey N, Berin MC. Pathogenesis of IgE-mediated food allergy and implications for future immunotherapeutics. Pediatr Allergy Immunol. 2021;32(7):1416–25. 10.1111/pai.13501
23. Burks AW, Sampson HA, Plaut M, Lack G, Akdis CA. Treatment for food allergy. J Allergy Clin Immunol. 2018;141(1):1–9. 10.1016/j.jaci.2017.11.004
24. de Silva D, Rodriguez Del Rio P, de Jong NW, Khaleva E, Singh C, Nowak-Wegrzyn A, et al. Allergen immunotherapy and/or biologicals for IgE-mediated food allergy: A systematic review and meta-analysis. Allergy. 2022;77(6):1852–62. 10.1111/all.15211
25. Nurmatov U, Dhami S, Arasi S, Pajno GB, Fernandez-Rivas M, Muraro A, et al. Allergen immunotherapy for IgE-mediated food allergy: A systematic review and meta-analysis. Allergy. 2017;72(8):1133–47. 10.1111/all.13124
26. Skripak JM, Nash SD, Rowley H, Brereton NH, Oh S, Hamilton RG, et al. A randomized, double-blind, placebo-controlled study of milk oral immunotherapy for cow’s milk allergy. J Allergy Clin Immunol. 2008;122(6):1154–60. 10.1016/j.jaci.2008.09.030
27. Pajno GB, Caminiti L, Ruggeri P, De Luca R, Vita D, La Rosa M, et al. Oral immunotherapy for cow’s milk allergy with a weekly up-dosing regimen: A randomized single-blind controlled study. Ann Allergy Asthma Immunol. 2010;105(5):376–81. 10.1016/j.anai.2010.03.015
28. Morisset M, Moneret-Vautrin DA, Guenard L, Cuny JM, Frentz P, Hatahet R, et al. Oral desensitization in children with milk and egg allergies obtains recovery in a significant proportion of cases. A randomized study in 60 children with cow’s milk allergy and 90 children with egg allergy. Eur Ann Allergy Clin Immunol. 2007;39(1):12–9.
29. Pouessel G, Lezmi G. Oral immunotherapy for food allergy: Translation from studies to clinical practice? World Allergy Organ J. 2023;16(2):100747. 10.1016/j.waojou.2023.100747
30. Yeung JP, Kloda LA, McDevitt J, Ben-Shoshan M, Alizadehfar R. Oral immunotherapy for milk allergy. Cochrane Database Syst Rev. 2012;11(11):CD009542. 10.1002/14651858.CD009542.pub2
31. Maeda M, Imai T, Ishikawa R, Nakamura T, Kamiya T, Kimura A, et al. Effect of oral immunotherapy in children with milk allergy: The ORIMA study. Allergol Int. 2021;70(2):223–8. 10.1016/j.alit.2020.09.011
32. Lee JH, Kim WS, Kim H, Hahn YS. Increased cow’s milk protein-specific IgG4 levels after oral desensitization in 7-to 12-month-old infants. Ann Allergy Asthma Immunol. 2013;111(6):523–8. 10.1016/j.anai.2013.09.001
33. Lodge CJ, Waidyatillake N, Peters RL, Netting M, Dai X, Burgess J, et al. Efficacy and safety of oral immunotherapy for peanut, cow’s milk, and hen’s egg allergy: A systematic review of randomized controlled trials. Clin Transl Allergy. 2023;13(7):e12268. 10.1002/clt2.12268
34. Ogata M, Kido J, Nakamura K. Oral immunotherapy for children with cow’s milk allergy. Pathogens. 2021;10(10). 10.3390/pathogens10101328
35. Paassilta M, Salmivesi S, Maki T, Helminen M, Korppi M. Children who were treated with oral immunotherapy for cow’s milk allergy showed long-term desensitisation seven years later. Acta Paediatr. 2016;105(2):215–9. 10.1111/apa.13251
36. Luyt D, Bravin K, Luyt J. Implementing specific oral tolerance induction to milk into routine clinical practice: Experience from first 50 patients. J Asthma Allergy. 2014;7:1–9. 10.2147/JAA.S53281
37. Keet CA, Seopaul S, Knorr S, Narisety S, Skripak J, Wood RA. Long-term follow-up of oral immunotherapy for cow’s milk allergy. J Allergy Clin Immunol. 2013;132(3):737–9.e6. 10.1016/j.jaci.2013.05.006
38. Manabe T, Sato S, Yanagida N, Hayashi N, Nishino M, Takahashi K, et al. Long-term outcomes after sustained unresponsiveness in patients who underwent oral immunotherapy for egg, cow’s milk, or wheat allergy. Allergol Int. 2019;68(4):527–8. 10.1016/j.alit.2019.02.012
39. Dantzer J, Dunlop J, Psoter KJ, Keet C, Wood R. Efficacy and safety of baked milk oral immunotherapy in children with severe milk allergy: A randomized, double-blind, placebo-controlled phase 2 trial. J Allergy Clin Immunol. 2022;149(4):1383–91 e17. 10.1016/j.jaci.2021.10.023
40. Epstein-Rigbi N, Goldberg MR, Levy MB, Nachshon L, Elizur A. Quality of life of food-allergic patients before, during, and after oral immunotherapy. J Allergy Clin Immunol Pract. 2019;7(2):429–36.e2. 10.1016/j.jaip.2018.06.016
41. Martorell A, Alonso E, Echeverria L, Escudero C, Garcia-Rodriguez R, Blasco C, et al. Oral immunotherapy for food allergy: A Spanish guideline. Immunotherapy Egg and Milk Spanish Guide (ITEMS Guide). Part I: cow milk and egg oral immunotherapy: introduction, methodology, rationale, current state, indications, contraindications, and oral immunotherapy build-up phase. J Investig Allergol Clin Immunol. 2017;27(4):225–37. 10.18176/jiaci.0177
42. Rodriguez Del Rio P, Alvarez-Perea A, Blumchen K, Caimmi D, Caubet JC, Konstantinopoulos AP, et al. Food immunotherapy practice: Nation differences across Europe, the FIND project. Allergy. 2022;77(3):920–32. 10.1111/all.15016
43. Laubach S, Kim EH, Greenhawt M, Bailey S, Anagnostou A. A review of shared decision-making, published protocols, and post-desensitization strategies in oral immunotherapy (OIT). Curr Allergy Asthma Rep. 2024;24(4):173–97. 10.1007/s11882-024-01132-2
44. Takaoka Y, Yajima Y, Ito YM, Kumon J, Muroya T, Tsurinaga Y, et al. Single-center noninferiority randomized trial on the efficacy and safety of low-and high-dose rush oral milk immunotherapy for severe milk allergy. Int Arch Allergy Immunol. 2020;181(9):699–705. 10.1159/000508627
45. Vazquez-Ortiz M, Turner PJ. Improving the safety of oral immunotherapy for food allergy. Pediatr Allergy Immunol. 2016;27(2):117–25. 10.1111/pai.12510
46. Meglio P, Bartone E, Plantamura M, Arabito E, Giampietro PG. A protocol for oral desensitization in children with IgE-mediated cow’s milk allergy. Allergy. 2004;59(9):980–7. 10.1111/j.1398-9995.2004.00542.x
47. Sato S, Nagakura KI, Yanagida N, Ebisawa M. Recent advances in oral immunotherapy for food allergies. Clin Rev Allergy Immunol. 2025;68(1):89. 10.1007/s12016-025-09108-4
48. Knol EF, de Jong NW, Ulfman LH, Tiemessen MM. Management of cow’s milk allergy from an immunological perspective: What are the options? Nutrients. 2019;11(11):2734. 10.3390/nu11112734
49. Nagakura KI, Sato S, Miura Y, Nishino M, Takahashi K, Asaumi T, et al. A randomized trial of oral immunotherapy for pediatric cow’s milk-induced anaphylaxis: Heated vs. unheated milk. Pediatr Allergy Immunol. 2021;32(1):161–9. 10.1111/pai.13352
50. Kiykim A, Karakoc-Aydiner E, Gunes E, Nain E, Ogulur I, Yazici D, et al. Evaluation of a standardized bakery product (SUTMEK) as a potential tool for baked-milk tolerance and immunotherapy research studies. Int Arch Allergy Immunol. 2019;178(1):1–9. 10.1159/000492824
51. Badina L, Burlo F, Belluzzi B, Babich S, Berti I, Barbi E. Life-threatening anaphylaxis in children with cow’s milk allergy during oral immunotherapy and after treatment failure. Immun Inflamm Dis. 2022;10(4):e607. 10.1002/iid3.607
52. Yanagida N, Sato S, Asaumi T, Okada Y, Ogura K, Ebisawa M. A single-center, case-control study of low-dose-induction oral immunotherapy with cow’s milk. Int Arch Allergy Immunol. 2015;168(2):131–7. 10.1159/000442157
53. Leonard SA, Laubach S, Wang J. Integrating oral immunotherapy into clinical practice. J Allergy Clin Immunol. 2021;147(1):1–13. 10.1016/j.jaci.2020.11.011
54. Staden U, Rolinck-Werninghaus C, Brewe F, Wahn U, Niggemann B, Beyer K. Specific oral tolerance induction in food allergy in children: Efficacy and clinical patterns of reaction. Allergy. 2007;62(11):1261–9. 10.1111/j.1398-9995.2007.01501.x
55. Berti I, Badina L, Cozzi G, Giangreco M, Bibalo C, Ronfani L, et al. Early oral immunotherapy in infants with cow’s milk protein allergy. Pediatr Allergy Immunol. 2019;30(5):572–4. 10.1111/pai.13057
56. Bone Calvo J, Clavero Adell M, Guallar Abadia I, Laliena Aznar S, Sancho Rodriguez ML, Claver Monzon A, et al. As soon as possible in IgE-cow’s milk allergy immunotherapy. Eur J Pediatr. 2021;180(1):291–4. 10.1007/s00431-020-03731-3
57. Hoshi-Funakawa M, Nagao M, Kawamoto N, Ohnishi H, Fujisawa T. Predictors of long-term desensitization in children treated with oral immunotherapy for food allergy: A real-world cohort study. J Clin Med. 2025;14(13):xxx. 10.3390/jcm14134727
58. Wood RA. Food allergen immunotherapy: Current status and prospects for the future. J Allergy Clin Immunol. 2016;137(4):973–82. 10.1016/j.jaci.2016.01.001
59. Dantzer JA, Lewis SA, Psoter KJ, Sutherland A, Frazier A, Richardson E, et al. Clinical and immunological outcomes after randomized trial of baked milk oral immunotherapy for milk allergy. JCI Insight. 2025;10(1):xxx. 10.1172/jci.insight.184301
60. Santos AF, Riggioni C, Agache I, Akdis CA, Akdis M, Alvarez-Perea A, et al. EAACI guidelines on the management of IgE-mediated food allergy. Allergy. 2025;80(1):14–36. 10.1111/all.16345
61. Kim S, Ahn K, Kim J. Practical issues of oral immunotherapy for egg or milk allergy. Clin Exp Pediatr. 2024;67(3):140–8. 10.3345/cep.2023.00234
62. Zhu H, Tang K, Chen G, Liu Z. Biomarkers in oral immunotherapy. J Zhejiang Univ Sci B. 2022;23(9):705–31. 10.1631/jzus.B2200047
63. Bartha I, Almulhem N, Santos AF. Feast for thought: A comprehensive review of food allergy 2021–2023. J Allergy Clin Immunol. 2024;153(3):576–94. 10.1016/j.jaci.2023.11.918
64. Bartha I, Boyd H, Foong RX, Krawiec M, Marques-Mejias A, Marshall HF, et al. The basophil activation test is the most accurate test in predicting allergic reactions to baked and fresh cow’s milk during oral food challenges. Allergy. 2025;80(10):2861–73. 10.1111/all.16675
65. Santos A, Dias A, Pinheiro JA. Predictive factors for the persistence of cow’s milk allergy. Pediatr Allergy Immunol. 2010;21(8):1127–34. 10.1111/j.1399-3038.2010.01040.x
66. Skripak JM, Matsui EC, Mudd K, Wood RA. The natural history of IgE-mediated cow’s milk allergy. J Allergy Clin Immunol. 2007;120(5):1172–7. 10.1016/j.jaci.2007.08.023
67. Wasserman RL. Long term oral immunotherapy management and assessment of success. J Food Allergy. 2022;4(2):102–5. 10.2500/jfa.2022.4.220015
68. US Food and Drug Administration (US FDA). FDA approves first medication to help reduce allergic reactions to multiple foods after accidental exposure. FDA, Silver Spring, MD; 2024.
69. Buono EV, Gianni G, Scavone S, Esposito S, Caffarelli C. Omalizumab and oral immunotherapy in IgE-mediated food allergy in children: A systematic review and a meta-analysis. Pharmaceuticals (Basel). 2025;18(3):xxx. 10.3390/ph18030437
70. Indolfi C, Perrotta A, Dinardo G, Klain A, Grella C, Palumbo P, et al. Omalizumab in food allergy in children: Current evidence and future perspectives. Life (Basel). 2025;15(5):xxx. 10.3390/life15050681