
Download
CASE REPORT
Is there hope for persistent airflow obstruction? From trial to practice: real-world efficacy of Tezepelumab in severe asthma with persistent airflow obstruction
Marta Bernaola*, Ana Umpiérrez
Allergy Department, Hospital Central de la Defensa Gómez Ulla, Madrid, Spain
Abstract
Background: Persistent airflow obstruction (PAO) is a challenging phenotype of severe asthma, characterized by accelerated lung function decline, increased morbidity, and poor response to conventional therapies. Tezepelumab, a human monoclonal antibody targeting thymic stromal lymphopoietin (TSLP), has demonstrated efficacy in reducing airway inflammation and improving lung function.
Objective: We report a real-world case of a 72-year-old male with long-standing severe allergic and eosinophilic T2 asthma, PAO, and multiple comorbidities, uncontrolled despite optimized therapy.
Material and Methods: Correlating with post hoc analyses of the PATHWAY and NAVIGATOR trials, Tezepelumab treatment resulted in significant clinical lessening of the condition.
In two trials, Tezepelumab reduced annualized asthma exacerbations by 61% in patients with PAO and improved lung function, with some patients no longer meeting PAO criteria. In our patient, 24 weeks of Tezepelumab therapy yielded a 370 mL increase in FEV1, only one mild exacerbation without hospitalization, decreased sputum production, and recovery of olfactory function.
Conclusion: These outcomes highlight the potential of Tezepelumab to address both lower and upper airway disease, likely through TSLP blockade and modulation of airway remodeling. Early intervention may be critical to maximize benefit, emphasizing the importance of individualized, multidisciplinary management and precision medicine in severe asthma with PAO.
Key words: persistent airflow obstruction (PAO), severe asthma, Tezepelumab, thymic stromal lymphopoietin (TSLP)
*Corresponding author: Marta Bernaola, Allergy Department, Hospital Central de la Defensa Gómez Ulla, Madrid, Spain. Email address: [email protected]
Received 23 October 2025; Accepted 2 December 2025; Available online 1 May 2026
Copyright: Bernaola M and Umpiérrez A
This open access article is licensed under Creative Commons Attribution 4.0 International (CC BY 4.0). http://creativecommons.org/licenses/by/4.0/
Introduction
Asthma is a chronic inflammatory disease of the airways characterized by variable airflow obstruction, which in some cases becomes persistent and poorly reversible, evolving into a condition known as chronic or persistent airflow obstruction (PAO).1,2 PAO is associated with accelerated decline in lung function, increased morbidity, and a less favorable response to conventional asthma therapies. Chronic inflammation, airway remodeling, and mucus impaction are the main pathophysiological mechanisms contributing to PAO.3
Tezepelumab, a human monoclonal antibody targeting thymic stromal lymphopoietin (TSLP), has demonstrated efficacy in reducing airway inflammation and improving lung function in patients with acute uncontrolled asthma. Recent clinical trials, including PATHWAY and NAVIGATOR, have shown that Tezepelumab significantly improves lung function and reduces asthma exacerbations, even in patients with PAO.4
This report summarizes the most recent findings on the efficacy of Tezepelumab and its potential role in modifying disease progression in severe asthma with PAO, correlating these results with a real-world clinical case.
Clinical Case
A 72-year-old male, ex-smoker for more than 40 years (pack-year index < 4), with a history of rhinitis, with significant bronchorrhea and mucus plugs, and persistent moderate-to-severe T2 asthma (allergic and eosinophilic). His asthma was secondary to sensitization to pollens, dust mites, and dog dander, as well as mild emphysema, moderate-to-severe positional obstructive sleep apnea with oximetric repercussions. The patient had a history of squamous cell carcinoma of the tonsil treated with surgery and radiotherapy, with permanent sequelae of anosmia and dysgeusia.
Despite long-term optimized controller treatment—including triple therapy (long-acting β2-agonist [LABA]/long-acting muscarinic antagonist [LAMA]/inhaled corticosteroid [ICS]), montelukast, oral antihistamines, and intranasal corticosteroids—the patient required rescue therapy with short-acting beta-agonists (SABA) three to four times daily, every day of the week. He had also received 5 years of specific immunotherapy against grass pollens. Since 2016, he experienced an average of two annual hospital admissions for bronchospasm requiring systemic corticosteroids. These exacerbations occurred in winter, coinciding with cypress pollination and respiratory infections, as well as in spring, associated with peaks of grass and olive pollens, with increased usage of SABA and oral corticosteroid.
Pulmonary function testing showed a post-bronchodilator (BD) forced expiratory volume in 1 s (FEV1)–forced vital capacity (FVC) ratio of <0.7, with negative BD reversibility and elevated fractional exhaled nitric oxide (FeNO) values. Peripheral blood eosinophilia was documented with counts ranging from 300 to 500 cells/μL.
Chest computed tomography (CT) scans without contrast, compared with a prior 2020 study, revealed no significant cervical, supraclavicular, axillary, or mediastinal lymphadenopathy (largest 9 mm pretracheal, stable). No pleural or pericardial effusion was identified. Stable paraseptal emphysema, fibrotic tracts, small bronchiectasis, and basal right atelectasis of chronic post-inflammatory appearance were observed. No significant pulmonary nodules, lytic or blastic skeletal lesions, or remarkable upper abdominal findings were detected. Radiological stability was confirmed, compared with 2020 study.
Based on these findings, controller treatment with Tezepelumab was initiated (Figures 1A and 1B; and 2A and 2B).
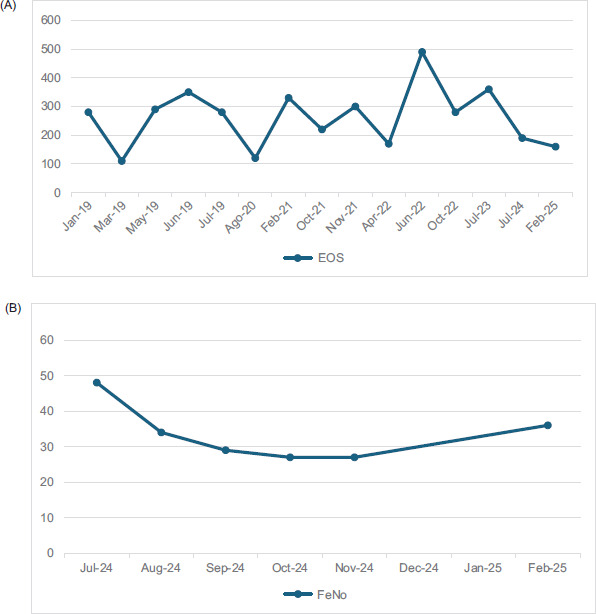
Figure 1 (A) Total peripheral blood eosinophil counts (BEC; cells/µL) before and after Tezepelumab treatment. (B) Monitoring of pre- and post-Tezepelumab exhaled nitric oxide (FeNO) levels. (Initiation of Tezepelumab in September 2024).
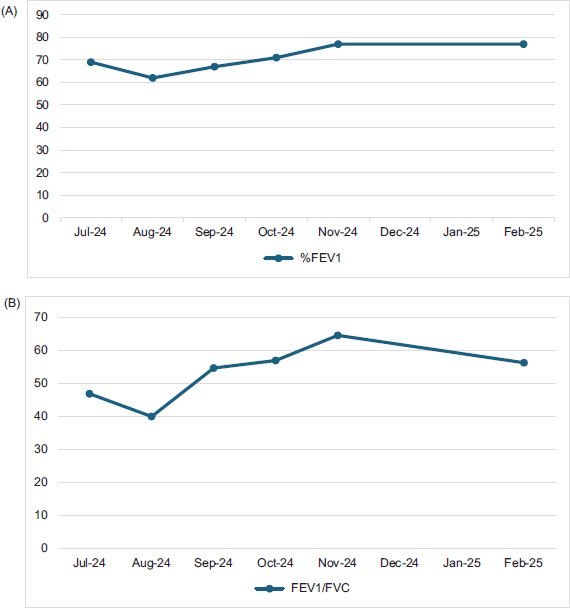
Figure 2 (A) Monitoring of lung capacity measured as a percentage (%) of FEV1 before and after Tezepelumab. (B) Monitoring of lung capacity measured using the Tiffeneau index (FEV1–FVC ratio) before and after tezepelumab. (Initiation of tezepelumab in September 2024).
Objective
To correlate the published post hoc analysis of the PATHWAY and NAVIGATOR trials with our real-world experience in a patient with long-standing severe allergic and eosinophilic T2 asthma and PAO.4
Materials and Methods
The study “Efficacy of Tezepelumab in patients with severe asthma and persistent airflow obstruction” analyzed the PATHWAY (phase 2b) and NAVIGATOR (phase 3) trials, which evaluated Tezepelumab in patients with uncontrolled severe asthma and PAO. Patients received Tezepelumab 210 mg or placebo every 4 weeks for 52 weeks.4
Results
After 52 weeks, Tezepelumab-treated patients showed significant improvement in lung function, compared to placebo, with and without PAO. Furthermore, Tezepelumab reduced the annualized asthma exacerbation rate by 61% in patients with PAO and by 56% in those without PAO. Patients with PAO receiving Tezepelumab were also more likely to no longer meet PAO criteria at study end (12.1% vs. 6.6% with placebo).4
In our patient, real-world results paralleled the trial findings. At 24 weeks, the patient gained 370 mL in FEV1, reduced maintenance medication, experienced only one mild exacerbation without requiring oral corticosteroids, and reported decreased sputum production, expulsion of mucus plugs, and recovery of smell. Moreover, he transitioned from severe to moderate PAO, defined as post-BD FEV1/FVC < 0.7, with severity classified as mild (60%–<70%), moderate (50%–<60%), or severe (<50%).4
Discussion
Asthma with PAO represents a clinical phenotype characterized by reduced post-BD FEV1/FVC, associated with accelerated lung function decline and increased morbidity.3 Although no universal definition exists, this analysis used the most common threshold: post-BD FEV1/FVC < 0.7 at baseline. Clinical overlap is notable between severe asthma with PAO and spirometric chronic obstructive pulmonary disease (COPD); however, the data demonstrate that patients with severe asthma and PAO, in particular, benefit from Tezepelumab.
Tezepelumab was selected because it targets a key epithelial alarmin involved in the early stages of inflammatory cascades across both type 2 (T2) and non-type 2 pathways. By acting upstream, Tezepelumab modulates multiple downstream mediators, including interleukin 4 (IL-4), IL-5, IL-13, and immunoglobulin E (IgE), which confers efficacy across a broad spectrum of asthma phenotypes, including allergic asthma. In the phase III NAVIGATOR trial, Tezepelumab demonstrated a significant reduction in annualized asthma exacerbation rates among patients with severe, uncontrolled asthma. This reduction was also observed in individuals with sensitization to perennial allergens and elevated serum IgE levels. Subgroup analyses further showed significant benefits in patients with allergic asthma, including improvements in lung function, symptom control, and reductions in biomarkers, such as blood eosinophils, fractional exhaled FeNO and total IgE. Unlike therapies that target a single cytokine, the upstream mechanism of Tezepelumab confers broader efficacy, making it a valuable therapeutic option for patients with allergic asthma, especially those who do not respond to anti-IgE or anti-IL-5 agents.4
This choice was primarily informed by evidence indicating that Tezepelumab offers greater efficacy compared with the anti-IgE agent omalizumab as a first-line biologic therapy in the absence of elevated levels of other T2 inflammatory biomarkers, including blood or sputum eosinophils and FeNO. In clinical trials, such as the LIBERTY ASTHMA QUEST study, dupilumab is shown to reduce annual asthma exacerbation rates and improve lung functioning in patients with elevated IgE levels and sensitization to perennial allergens. These effects are further enhanced in individuals with high blood eosinophil counts (BEC) or elevated FeNO.4
Post hoc analyses of PATHWAY and NAVIGATOR confirmed that Tezepelumab improved lung function and reduced exacerbations, compared with placebo in uncontrolled severe asthma patients both with and without PAO. Lung function improvements relative to placebo were greater in PAO patients, especially those with elevated type 2 inflammation (high eosinophils or FeNO). Gains in post-BD FEV1 and FVC suggest benefits beyond β-agonist bronchodilation.4
Airway remodeling in PAO is characterized by increased airway smooth muscle, fibrosis, and goblet cell hyperplasia, driven in part by chronic inflammation. TSLP is implicated in multiple inflammatory and remodeling pathways, including airway smooth muscle–mast cell interactions.5–7 Although the precise mechanism by which Tezepelumab improves lung function remains unclear, its broad inhibition of TSLP may explain these effects.8,9 Furthermore, it may be related to the multiple pathways through which TSLP contributes to inflammation and airway remodeling. In addition to inducing both type 2 and non-type 2 inflammation, increased TSLP expression is demonstrated in airway smooth muscles in asthma, where it may play a role in the interaction between smooth muscle cells and mast cells.10–13
Exacerbation rates were higher in placebo-treated PAO patients than in those without PAO, yet Tezepelumab reduced rates in both groups to similar levels.4 In line with the overall findings of the NAVIGATOR trial,14 greater reductions were observed in patients with higher baseline biomarkers (BEC ≥ 300/μL; FeNO ≥ 25 ppb). The most pronounced benefits occurred in patients with more severe PAO (post-BD FEV1/FVC < 60%).
Clinically meaningful improvements in pre-BD FEV1 with Tezepelumab versus placebo were observed in patients with elevated inflammatory biomarkers, irrespective of the presence of PAO. The greatest reductions in exacerbations over 52 weeks were observed in patients with more severe PAO (post-BD FEV1/FVC < 50% and 50%–<60%), compared to those with milder obstruction (post-BD FEV1/FVC 60%–<70% and ≥70%).
Although patients with baseline PAO showed consistent clinical benefits, only a minority no longer met PAO criteria after 52 weeks of treatment. Those who achieved this transition tended to be younger and had a shorter disease duration.4 These findings suggest that earlier initiation of Tezepelumab may be critical to prevent irreversible airway remodeling. However, consideration must also be afforded to optimizing background therapy, ensuring treatment adherence, and evaluating the cost-effectiveness of introducing biologics at an earlier stage.
Limitations include the exploratory nature of the analysis and insufficient statistical power to specifically assess Tezepelumab’s impact in PAO subgroups; so, findings should be interpreted as descriptive.4
Conclusions
Treatment with Tezepelumab improved lung function, including post-BD parameters, and reduced asthma exacerbations compared with placebo in patients with uncontrolled severe asthma and PAO, a phenotype that is often challenging to manage. These improvements further support the efficacy of Tezepelumab across a broad population of patients with severe asthma and suggest potential effects on airway remodeling.
In our patient, the post hoc findings were not only replicated but exceeded, with the patient achieving a 370-mL improvement in FEV1 and an even greater reduction in exacerbation frequency, as only one mild exacerbation occurred during pollen season, without hospitalization—a marked contrast to his pre-treatment history.
Additionally, he experienced substantial decrease in upper airway disease, regaining his sense of smell (e.g., detecting perfume and coffee) along with reduced rhinorrhea and sputum production, which allowed decreased use of intranasal corticosteroids. These observations were consistent with the findings of Nordenmark et al.,5 who reported that Tezepelumab treatment was associated with a reduction in mucus plugs in patients with uncontrolled moderate-to-severe asthma. This supports the concept that mucus plugging in patients with chronic or PAO may represent a treatable trait addressed through TSLP blockade.
The complexity of these patients underscores the importance of individualized assessment by a multidisciplinary team and the application of precision medicine for optimal outcomes.
Finally, these findings support the hypothesis that early initiation of Tezepelumab may be critical in preventing irreversible airway remodeling, provided that other key factors—such as optimization and adherence to background therapy and the cost-effectiveness of early biologic intervention—are also considered.
Mandatory Disclosure on Use of Artificial Intelligence
The authors declare that no AI-assisted tools were used in the preparation of this manuscript. All references have been manually verified for accuracy and relevance.
Author Contributions
Both authors contributed equally to this article.
Conflict of Interest
Authors had no conflict of interest to disclose. The patient consented to the publication of the case. Written informed consent was obtained from the patient for the publication of any potentially identifiable images or data included in this article.
Funding
The authors declared that no financial support was received for the research, authorship, and/or publication of this article.
REFERENCES
1 Bumbacea D, Campbell D, Nguyen L, et al. Parameters associated with persistent airflow obstruction in chronic severe asthma. Eur Respir J. 2004;24:122–8. 10.1183/09031936.04.00077803
2 Global Initiative for Asthma. Global strategy for asthma management and prevention [Internet]. [cited 2023]. Available from: https://ginasthma.org
3 Konstantellou E, Papaioannou AI, Loukides S, et al. Persistent airflow obstruction in patients with asthma: Characteristics of a distinct clinical phenotype. Respir Med. 2015;109:1404–9. 10.1016/j.rmed.2015.09.009
4 Israel E, Castro M, Ambrose CS, et al. Efficacy of tezepelumab in patients with severe asthma and persistent airflow obstruction. ERJ Open Res. 2024;10(6):164-2024 10.1183/23120541.00164-2024
5 Nordenmark L, Hellqvist A, Emson C, et al. Tezepelumab and mucus plugs in patients with moderate-to-severe asthma. NEJM Evid. 2023;2(10):EVIDoa2300135. 10.1056/EVIDoa2300135.
6 Fehrenbach H, Wagner C, Wegmann M. Airway remodeling in asthma: What really matters. Cell Tissue Res. 2017;367:551–69. 10.1007/s00441-016-2566-8.
7 Joseph C, Tatler AL. Pathobiology of airway remodelling in asthma: The emerging role of integrins. J Asthma Allergy. 2022;15:595–610. 10.2147/JAA.S267222
8 Hough KP, Curtiss ML, Blain TJ, et al. Airway remodeling in asthma. Front Med (Lausanne). 2020;7:191. 10.3389/fmed.2020.00191
9 Varricchi G, Ferri S, Pepys J, et al. Biologics and airway remodeling in severe asthma. Allergy 2022;77:3538–52. 10.1111/all.15473
10 Gauvreau GM, Sehmi R, Ambrose CS, et al. Thymic stromal lymphopoietin: Its role and potential as a therapeutic target in asthma. Expert Opin Ther Targets. 2020;24:777–92. 10.1080/14728222.2020.1783242.
11 Cao L, Liu F, Liu Y, et al. TSLP promotes asthmatic airway remodeling via p38-STAT3 signaling pathway in human lung fibroblast. Exp Lung Res. 2018;44:288–301. 10.1080/01902148.2018.1536175
12 Gandhi NA, Bennett BL, Graham NM, et al. Targeting key proximal drivers of type 2 inflammation in disease. Nat Rev Drug Discov. 2016;15:35–50. 10.1038/nrd4624
13 Kaur D, Doe C, Woodman L, et al. Mast cell-airway smooth muscle crosstalk: The role of thymic stromal lymphopoietin. Chest. 2012;142:76–85. 10.1378/chest.11-1782
14 Menzies-Gow A, Corren J, Bourdin A, et al. Tezepelumab in adults and adolescents with severe, uncontrolled asthma. N Engl J Med. 2021;384:1800–09. 10.1056/NEJMoa2034975