
Download
REVIEW ARTICLE
Environmental exposure to allergens in the home and analysis instruments: a scoping review
Lívia Maria Nunes Campeloa*, Georgia Veras de Araújo Gueiros Liraa,b, Emanuel Savio Cavalcanti Sarinhoa,b
aPostgraduate Programme in Child and Adolescent Health, Federal University of Pernambuco, Recife, PE, Brazil
bAllergy and Clinical Immunology Research Centre, Federal University of Pernambuco, Recife, PE, Brazil
Abstract
The objective was to identify possible validated instruments used to assess environmental exposure to allergens in the home. A scoping review was conducted including full articles published in Portuguese, English, and Spanish, up to July 2025, without a time limit, in the databases MEDLINE/PubMed, EMBASE, Scopus, CINAHL, and Web of Science databases. Three studies, published between 1999 and 2022, comprised the review. Three validated instruments were identified: one restricted to criterion validation and two with more comprehensive validation (construct, content, criterion, and reliability assessment). The main respiratory allergens assessed by the instruments were house dust mites, animal epithelia (particularly cats and dogs), cockroaches, and fungi. The review identified a small number of instruments in the literature, including a single instrument capable of assessing exposure to allergens in the home without the need for targeted observation, using direct interviews with patients as the assessment method. The results presented indicate a shortage of validated, widely used instruments worldwide to investigate the home environment of patients with respiratory allergies, thereby compromising the development of necessary guidelines to mitigate allergen exposure, a fundamental principle of all allergy treatment.
Key words: allergens, environmental exposure, home environment, surveys and questionnaires, validation study
*Corresponding author: Lívia Maria Nunes Campelo, Postgraduate Programme in Child and Adolescent Health, Federal University of Pernambuco. Av. Prof. Morais Rego, 1235 – City University student, Recife - PE, Brazil. Email address: [email protected]
Received 21 October 2025; Accepted 13 January 2026; Available online 1 May 2026
Copyright: Campelo LMN, et al.
This open access article is licensed under Creative Commons Attribution 4.0 International (CC BY 4.0). http://creativecommons.org/licenses/by/4.0/
Introduction
Exposure to environmental allergens plays a crucial role in the development and exacerbation of allergic diseases such as rhinitis, asthma, and atopic dermatitis, affecting individuals of all age groups and representing a significant public health problem worldwide.1,2 Generally, aeroallergens are distributed in outdoor environments, most frequently as fungi and pollen, and indoor (intra-domestic) environments, such as house dust mites, cat and dog dander, and cockroaches.3,4 In addition to allergens, other agents exist that do not cause allergies but exacerbate allergic symptoms such as irritants, which trigger the release of inflammatory substances by mast cells.5 Among the main aggravating factors are tobacco smoke, perfume odours, cleaning products, temperature changes, among others.5-7
Another almost or even imperceptible agent, yet of great impact on allergic conditions, is microplastics. Studies indicate that exposure to microplastics alters the alveolar structure and barrier function of the respiratory tract, thereby facilitating the penetration of allergens, irritants, and microorganisms, thereby enabling the development of a chronic inflammatory process.8,9 In the indoor environment, there are various direct and indirect sources of microplastics, such as personal hygiene products, paints, artificial turf, abrasion of floors, furniture, and textiles.10,11
The investigation of which sources of allergens, irritants, and pollutants are present in greater quantities in the patient’s home, and which worsen disease symptoms, is of fundamental importance for educating allergic patients about environmental control. Measures to prevent exposure to common allergens in the individual’s living environment constitute an adjuvant measure to pharmacological treatment in allergies.12,13 However, this environmental control may not always be effective given the population’s socioeconomic inequalities. While some families reside in ventilated homes with washable floors, others live in precarious dwellings with humidity, dust accumulation, and inadequate ventilation.11
Under these conditions, implementing environmental control measures, which are essential for reducing exposure to domestic allergens, poses a significant challenge. Therefore, it is essential for health professionals to understand the environment in which these individuals are situated, whether through direct observation or investigation, using a sensitive approach that considers the social context and seeks feasible strategies adapted to local reality.
To support this inspection, we can use instruments to assess and measure allergen exposure. Several approaches can be used, such as collecting household dust samples, laboratory analyses (ELISA and PCR), and environmental sensors as investigative alternatives; however, questionnaires constitute useful, indispensable, and easily accessible instruments for most health professionals.14-15 Therefore, this scoping review gathered validated instruments available in the literature for assessing domestic allergen exposure, allowing health professionals to choose the most appropriate option for the patient’s reality and, consequently, implement effective strategies to reduce exposure, decrease the burden of allergic diseases, reduce healthcare costs, and promote a better quality of life for patients.
Methods
A scoping review was conducted following the methodological recommendations of the Joanna Briggs Institute (JBI) and the study selection process according to the recommendations of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA-ScR) – an extension for scoping reviews.16,17
Search strategy
For the formulation of the guiding question, the Population, Concept, Context (PCC) acronym was considered, with P (general population), C (instruments designed for environmental allergen exposure assessment), and C (home environment). Based on these definitions, the question guiding the review was to identify which instruments available in the literature are being used to assess allergen exposure in the home.
Searches for eligible studies were conducted up to July 2025, in the following databases: MEDLINE/PubMed, EMBASE, Scopus, CINAHL, and Web of Science. Adjustments to the search strategy were made according to the specificities of each database, maintaining a similar combination of descriptors, as shown in Table 1.
Table 1 Search strategy in each database.
| Database | Search Strategy |
|---|---|
| MEDLINE/PubMed | ((((“Survey Research”[Title/Abstract] OR Questionnaire[Title/Abstract] OR “Survey Methods”[Title/Abstract] OR “Survey Methodology”[Title/Abstract] OR Tools[Title/Abstract] OR Measures[Title/Abstract] OR Scales[Title/Abstract] OR Checklists[Title/Abstract] OR Instruments[Title/Abstract]) AND (“Environmental Exposure”[Title/Abstract] OR “Environmental contamination”[Title/Abstract] OR “Exposure to environmental factors”[Title/Abstract] OR “Ambient exposure”[Title/Abstract] OR “Exposure to allergens”[Title/Abstract] OR “Household environmental exposure”[Title/Abstract] OR “Indoor exposure”[Title/Abstract] OR “Home exposure”[Title/Abstract] OR “Residential exposure”[Title/Abstract] OR “Domestic exposure”[Title/Abstract])) AND (“Place of residence”[Title/Abstract] OR “Residential address”[Title/Abstract] OR “Residence Characteristic”[Title/Abstract] OR “Domicile Domiciles”[Title/Abstract] OR Household[Title/Abstract] OR Home[Title/Abstract] OR Residence[Title/Abstract] OR Habitation[Title/Abstract] OR “Domestic environment”[Title/Abstract])) AND (Allergen[Title/Abstract] OR “allergic agent”[Title/Abstract])) |
| CINAHL | (“Surveys and Questionnaires” OR “Survey Research” OR questionnaire OR “Survey Methods” OR “Survey Methodology” OR Tools OR Measures OR Scales OR Checklists OR Instruments) AND (“Environmental Exposure”OR “Environmental contamination” OR “Exposure to environmental factors” OR “Ambient exposure” OR “Exposure to allergens” OR “Household environmental exposure” OR “Indoor exposure” OR “Home exposure” OR “Residential exposure” OR “Domestic exposure”) AND (“Place of residence” OR “residential address” OR “Residence Characteristic” OR “Domicile Domiciles” OR Household OR Home OR Residence OR Habitation OR “Domestic environment”) AND (Allergen OR “allergic agent”) |
| Scopus | (TITLE-ABS-KEY (“Surveys and Questionnaires” OR “Survey Research” OR questionnaire OR “Survey Methods” OR “Survey Methodology” OR tools OR measures OR scales OR checklists OR instruments) AND TITLE-ABS-KEY (“Environmental Exposure” OR “Environmental contamination” OR “Exposure to environmental factors” OR “Ambient exposure” OR “Exposure to allergens” OR “Household environmental exposure” OR “Indoor exposure” OR “Home exposure” OR “Residential exposure” OR “Domestic exposure”) AND TITLE-ABS-KEY (“Place of residence” OR “residential address” OR “Residence Characteristic” OR “Domicile Domiciles” OR household OR home OR residence OR habitation OR “Domestic environment”) AND TITLE-ABS-KEY (allergen OR “allergic agent”)) |
| Web of Science | (“Surveys and Questionnaires” OR “Survey Research” OR questionnaire OR “Survey Methods” OR “Survey Methodology” OR Tools OR Measures OR Scales OR Checklists OR Instruments) AND (“Environmental Exposure”OR “Environmental contamination” OR “Exposure to environmental factors” OR “Ambient exposure” OR “Exposure to allergens” OR “Household environmental exposure” OR “Indoor exposure” OR “Home exposure” OR “Residential exposure” OR “Domestic exposure”) AND (“Place of residence” OR “residential address” OR “Residence Characteristic” OR “Domicile Domiciles” OR Household OR Home OR Residence OR Habitation OR “Domestic environment”) AND (Allergen OR “allergic agent”) |
| EMBASE | (surveys:ab,ti AND questionnaires:ab,ti OR ‘survey research’:ab,ti OR questionnaire:ab,ti OR ‘survey methods’:ab,ti OR ‘survey methodology’:ab,ti OR tools:ab,ti OR measures:ab,ti OR scales:ab,ti OR checklists:ab,ti OR instruments:ab,ti) AND (‘environmental exposure’:ab,ti OR ‘environmental contamination’:ab,ti OR ‘exposure to environmental factors’:ab,ti OR ‘ambient exposure’:ab,ti OR ‘exposure to allergens’:ab,ti OR ‘household environmental exposure’:ab,ti OR ‘indoor exposure’:ab,ti OR ‘home exposure’:ab,ti OR ‘residential OR ‘domestic exposure’:ab,ti) AND (‘place of residence’:ab,ti OR ‘residential address’:ab,ti OR ‘residence characteristic’:ab,ti OR ‘domicile domiciles’:ab,ti OR household:ab,ti OR home:ab,ti OR residence:ab,ti OR habitation:ab,ti OR ‘domestic environment’:ab,ti) AND (allergen:ab,ti OR ‘allergic agent’:ab,ti) |
Eligibility criteria
Inclusion criteria were original full-text studies addressing validated instruments for assessing environmental allergen exposure in the home; literature reviews; and theses and dissertations. Studies in Portuguese, English, or Spanish were included. Pilot studies, case/experience reports, letters, editorials, and conference proceedings were excluded.
Study selection and data extraction
Study selection occurred in four stages: identification of articles in databases, duplicate removal, title and abstract screening, and full-text reading with data stratification. Considering the inclusion criteria, two researchers (L.M.N.C. and G.V.A.G.L.) were responsible for reading the titles and abstracts of the works to determine which would be read in full. This stage was performed independently to enable comparison of the included articles. In case of disagreement, a third author (E.S.C.S.) was called upon for consensus. The study selection process is presented in Figure 1, according to the recommendations of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA).
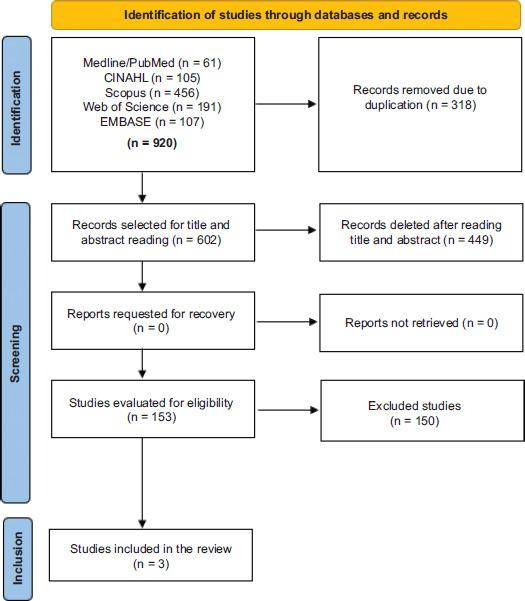
Figure 1 Flowchart of the study identification, selection, and inclusion process, developed based on the PRISMA-ScR recommendation. n = the number of studies.
For data collection, a form was developed covering the following items: author, year of publication, country, study objective, population, instrument name, instrument validation methodology, domains/sections, and method of instrument assessment.
Results
A total of 920 studies were identified in the databases, with 318 duplicate publications removed. After title and abstract screening, 449 studies were excluded, and 153 full texts were assessed, resulting in 150 exclusions for not meeting eligibility criteria. Thus, three articles were included for data extraction. Figure 1 illustrates the study selection process. Table 2 presents the general characteristics of the included instruments.
Table 2 General characteristics of aeroallergen assessment instruments.
| Author/Country | Instrument | Assessment | Response | Domains/Sections | Validation method |
|---|---|---|---|---|---|
| Dharmage et al.18 (Australia) | Home Visit Report (originally developed by C. Luczynska) | Interviewer-administered questionnaire + direct observation | Alternative (yes/no) + complementary quantitative questions + observational items completed by the interviewer | House structure, heating systems, ventilation, floor coverings, bedding, pets, vacuum cleaner, gas oven or stove, cleaning material, humidity, and mould. (Total of 44 questions) | Construct validation Criterion validation Reliability assessment (test-retest) |
| Gehring et al.19 (USA) | Questionnaire of cat and dog ownership and presence of cockroaches | Interviewer-administered questionnaire + direct observation | Alternatives (yes/no) + complementary quantitative questions (e.g., number of animals, time since last presence) | Current and past ownership of cats and dogs, number of animals, animal access to the baby’s room, visual presence of household pests, such as cockroaches. (Total of 4 questions) | Criterion validation |
| De Souza et al.20 (Brazil) | Questionnaire to Qualify the Environment Exposure to Aeroallergens - Q2E2a | Interviewer-administered questionnaire | Alternatives (yes/no). With scoring for each item and exposure classification according to total points | Environment ventilation, household dust, pets/insects, and household cleaning. (Total of 29 questions) | Content validation Criterion validation Reliability assessment (test-retest) |
Discussion
It is essential that environmental control receives its full value in the treatment of patients with respiratory allergies, given the prevention of respiratory complications and the rationalisation of pharmacological therapies that such practice can achieve. To achieve this environmental control, a first step for health professionals is to understand the environment in which the allergic individual lives, either through a structured interview or a home visit. Therefore, environmental assessment instruments constitute an important strategy for controlling allergies, especially respiratory ones.
Mapping instruments for assessing environmental allergen exposure in the home guided this scoping review. This is the first study to compile only validated instruments suitable for use, which can guide the production of relevant knowledge for the planning of the treatment of allergic patients. A limited number of instruments assessing environmental allergen exposure in the home were identified. During the article screening process, a significant number of studies that used unvalidated questionnaires for home environmental assessment were identified, consistent with Punyadasa et al.’s scoping review.21
The temporal evolution of indoor environments significantly challenges the contemporary applicability of traditional environmental assessment instruments in managing respiratory allergies. Alterations in housing characteristics, such as the introduction of novel building materials that emit diverse volatile organic compounds, and shifts in ventilation strategies that prioritise energy efficiency over natural ventilation profoundly modify indoor aeroallergen and pollutant exposure profiles. Furthermore, evolving domestic habits, including widespread air conditioning use, reshape the spectrum and concentration of immunological triggers within residential settings. Consequently, older tools may inadequately capture the nuanced environmental dynamics imperative for effective patient care, necessitating the development and rigorous validation of updated instruments tailored to current indoor conditions to optimize therapeutic interventions and mitigate disease exacerbation.22
Simultaneously, the incorporation of current and escalating exposures to microplastics, extreme weather events, and rising indoor temperatures and humidity would substantially reinforce the justification for developing new assessment tools. These emerging factors, intrinsically linked to asthma, serve as distinct immunological triggers not currently addressed by existing instruments. Emphasising their pervasive nature and pathophysiological effects highlights the critical inadequacy of current questionnaires and underscores the urgent need for robust, multifactorial tools capable of accurately characterising the complex indoor exposome, which is essential for effective clinical management and preventive strategies in allergic respiratory diseases.23
In this context, four observation and distinction points for the instruments were outlined: the investigation items comprising each questionnaire; their applicability and facilitators for use in clinical practice; the possibility of classifying the patient’s home environment; and the instrument’s construction and validation process. According to the analysed studies, the main allergens assessed by the instruments were house dust mites, animal dander (particularly cats and dogs), cockroaches, and fungi. These allergens are established in the literature as the most relevant in domestic environments in the context of sensitization and exacerbation of respiratory allergic diseases, such as allergic rhinitis and asthma.13 The studies by Solarz et al. and Salo et al. corroborate these findings, highlighting Dermatophagoides genus mites, Canis familiaris (Can f 1) and Felis domesticus (Fel d 1) dander, as well as proteins such as Bla g 1 from the German cockroach, as important immunological triggers for atopic individuals.24-25
Regarding the investigation items comprising the instruments, we observed that the Home Visit Report and the Questionnaire to Qualify the Environment Exposure to Aeroallergens - Q2E2a are more comprehensive, as they assess a wider range of domestic allergens, including dust, mould, pets, and cleaning materials. In contrast, the Questionnaire of Cat and Dog Ownership and Presence of Cockroaches is restricted to investigating only these animals within the domestic sphere.18–20
For practice, among the instruments, the Home Visit Report appears more extensive due to the number of items, making its application more time-consuming, in addition to requiring direct observation by the interviewer.18 The Questionnaire of Cat and Dog Ownership and Presence of Cockroaches requires less application time, as it consists of only four questions.19 According to the study on the Questionnaire to Qualify the Environment Exposure to Aeroallergens—Q2E2a, its application is broad and does not require direct home observation.20
Regarding environmental classification, only the Questionnaire to Qualify the Environment Exposure to Aeroallergens—Q2E2a allows for estimating, through a sum of points, whether the environment has allergen control in the home. The Home Visit Report is more focused on residential characterization. The authors of the Questionnaire of Cat and Dog Ownership and Presence of Cockroaches concluded in their study that, for epidemiological purposes, objective measures (dust/ELISA) are needed, in addition to the questionnaire, to predict animal allergen levels in the home.18–20
The Home Visit Report instrument, during its construction, underwent construct, criterion, and reliability assessments, demonstrating methodological robustness through objective measures and appropriate statistical approaches.18 However, even following rigorous and well-delineated steps, a significant gap, such as content validation, prevents the instrument from being considered psychometrically complete.
Studies on instrument development and validation indicate that a robust approach should include reliability assessment and multiple types of validation, including construct, content, and criterion, thereby ensuring methodological rigour and applicability in clinical and epidemiological contexts.26,27 It is noteworthy that reliability and validity are not fixed properties; they vary with the study’s purpose and context. Nevertheless, these limitations do not invalidate the instrument. The Home Visit Report proves valid and reliable for assessing residential characteristics associated with environmental allergen exposure. With alignment to more comprehensive validation processes, the instrument can be adapted to different populations and epidemiological contexts.
The Questionnaire of Cat and Dog Ownership and Presence of Cockroaches was conducted only with criterion validation, comparing self-reported responses with environmental measurements of household dust samples by the ELISA method. Its results demonstrated that self-reported questionnaire data have predictive capacity for accentuated exposures (levels above the upper cut-off point) but low sensitivity for low-intensity exposures.19 Although the study was conducted with a significant population sample and data were reliably obtained through laboratories, the absence of stages such as content validation, internal consistency, and temporal reliability indicates a limitation of the instrument regarding a complete psychometric validation. Thus, it is recommended that the questionnaire incorporate additional validation stages in future research to enhance its applicability.
On the other hand, the Questionnaire to Qualify the Environment Exposure to Aeroallergens—Q2E2a presented a more comprehensive validation process, including essential stages such as content validity, criterion validity, and test–retest reliability. The development of the items was based on a literature review and clinical experience, followed by expert review and a pilot test, which ensured the relevance and clarity of the items. In the last stage, the comparison between self-reported responses and photographic inspection of the environment, as well as the use of test–retest, reinforced methodological adequacy, which resulted in significant concordance indices for most items.20 Regarding the Q2E2a instrument, the absence of a laboratory gold standard for criterion validation is notable. However, its comparison with photographic home-environment inspection, which demonstrated adequate validity for exposure characterisation, offers a pragmatically acceptable alternative. In real clinical contexts, where efficiency and accessibility are paramount, such simplified approaches can be preferable for optimising consultation time and reducing costs. This balance between methodological rigour and practical feasibility is fundamental for effective assessment tools.
Some important considerations and limitations were identified in this review. This is the first study to broadly assess the availability of validated instruments for measuring exposure to and environmental characterisation of allergens and irritants in the home, with insights into their development and content. Furthermore, we did not identify in the literature any cross-cultural validation in other countries/languages for the instruments included in this review. Another strength of our review is the distribution of instrument origins: two are from high-income countries and one from a low-income developing country, allowing readers to select an appropriate tool for their context, with characteristics similar to their locality. Regarding limitations, the limited number of instruments available precluded comparison of the realities and contexts in which the instruments were originally validated. Another limitation was the noncoverage of instruments in languages other than Portuguese, English, and Spanish. It is worth emphasising that the review depends on scientific publications available in databases. In some cases, possibly validated instruments used in healthcare service practice may not be available in the literature and, for this reason, were not included in this review.
Given the main characteristics and validity evidence of each instrument, we enable health professionals to decide which instrument suits their local context, resources, and preferences. We highlight the importance of instruments such as the Q2E2a, which can reduce costs and assistive time, as it allows for assessment through a single brief interview without the need for direct observation of the home environment.20
Future Perspective
Over the next 10 years, advances are expected in the standardisation of instruments for assessing environmental exposure to allergens in the home. The incorporation of technologies such as low-cost portable environmental monitoring devices and mobile applications integrated with medical databases will increase the accuracy of these instruments. In addition, machine learning and artificial intelligence can assist in the analysis of large volumes of environmental and medical data, allowing for the recognition of exposure patterns by region or type of housing. This perspective will favour the development of hybrid scales (self-administered and observational), promoting greater comparability between international studies and reinforcing policies for the prevention and management of allergic diseases.
Conclusions
This scoping review revealed a notable scarcity of validated and comprehensively used instruments for assessing environmental allergen exposure in the home, with only three identified in the literature. These instruments showed heterogeneity in psychometric validation processes, ranging from restricted criterion validation to more comprehensive approaches, although one of them stands out for allowing assessment through direct interview, eliminating the need for on-site observation and optimising care flows and operational costs. This methodological gap underscores the need to increasingly use instruments that provide effective guidance from health professionals to mitigate exposure to inhaled allergens and irritants, a fundamental pillar of the treatment of allergic diseases, particularly respiratory ones. Consequently, future investigations should focus on the development of new, robustly validated instruments across multiple contexts, on the cross-cultural validation of existing questionnaires, and on the implementation of tools that facilitate environmental assessment, with the aim of improving intra-domestic control at each consultation and, thus, enhancing the quality of life of allergic patients.
Acknowledgements
We would like to thank the Postgraduate Program in Child and Adolescent Health at the Federal University of Pernambuco, linked to the Coordination for the Improvement of Higher Education Personnel – CAPES and the National Council for Scientific and Technological Development – CNPq.
Mandatory Disclosure on Use of Artificial Intelligence
The authors declare that no artificial intelligence tools were used in the preparation of the manuscript (Environmental exposure to allergens in the home and analysis instruments: a scoping review). All references were manually checked for accuracy and relevance.
Author Contributions
All authors contributed equally to this article.
Conflicts of Interest
The authors declare no potential conflicts of interest with respect to research, authorship, and/or publication of this article.
Funding
All authors contributed equally to this article.
REFERENCES
1 Rong CWW, Salleh H, Nishio H, Lee M. The impact of increasing ambient temperature on allergic rhinitis: a systematic review and meta-analysis of observational studies. Sci Total Environ. 2024;947. 10.1016/j.scitotenv.2024.174348
2 Conroy ER, Peterson R, Phipatanakul W, Sheehan WJ. Increasing awareness regarding the relationship between environmental exposures and allergic disease. J Allergy Clin Immunol. 2024;154(4):874–81. 10.1016/j.jaci.2024.08.008
3 Pattanayak S, Dinda SK, Hazra S, Mukhopadhyay R, Samanta S, Dey S, et al. Confronting allergies: strategies for combating pollution and safeguarding our health. Front Allergy. 2025;5:1521072. 10.3389/falgy.2024.1521072
4 Luyten A, Bürgler A, Glick S, Kwiatkowski M, Gehrig R, Beigi M, et al. Ambient pollen exposure and pollen allergy symptom severity in the EPOCHAL study. Allergy. 2024;79(7):1908–20. 10.1111/all.16130
5 Mwanga HH, Dumas O, Migueres N, Moual NL, Jeebhay MF. Airway diseases related to the use of cleaning agents in occupational settings. J Allergy Clin Immunol Pract. 2024;12(8):1974–86. 10.1016/j.jaip.2024.02.036
6 Muta H, Noda T. Survey of secondhand smoke for 3-year-old children in the current era of new tobacco products. Acta Paediatr. 2025;114(6):1405–13. 10.1111/apa.17584
7 Eguiluz-Gracia I, Mathioudakis AG, Bartel S, Vijverberg SJH, Fuertes E, Comberiati P, et al. The need for clean air: the way air pollution and climate change affect allergic rhinitis and asthma. Allergy. 2020;75(9):2170–84. 10.1111/all.14177
8 Urrutia-Pereira M, Guidos-Fogelbach G, Chong-Neto HJ, Solé D. Microplastics exposure and immunologic response. Alergol Inmunol Clin (Madr). 2023;51(5):57–65. 10.15586/aei.v51i5.834
9 Gou Z, Wu H, Li S, Liu Z, Zhang Y. Airborne micro-and nanoplastics: emerging causes of respiratory diseases. Part Fibre Toxicol. 2024;21:50. 10.1186/s12989-024-00613-6
10 Gaylarde CC, Baptista Neto JA, da Fonseca EM. Indoor airborne microplastics: human health importance and effects of air filtration and turbulence. Microplastics. 2024;3(4):653–70. 10.3390/microplastics3040040
11 Din KS, Khokhar MF, Parvez S, Niazi MBK. Emerging environmental challenge: a critical review of airborne microplastics. Environ Res Commun. 2024;6(9):1–24 10.1088/2515-7620/ad75eb
12 Tomé M, Lourenço O. Avoidance measures for patients with allergic rhinitis: a scoping review. Children (Basel). 2023;10(2):300. 10.3390/children10020300
13 Grant TL, Wood RA, Chapman MD. Indoor environmental exposures and their relationship to allergic diseases. J Allergy Clin Immunol Pract. 2023;11(10):2963–70. 10.1016/j.jaip.2023.08.034
14 Putcha N, Woo H, McCormack MC, Fawzy A, Romero K, Davis MF, et al. Home dust allergen exposure is associated with outcomes among sensitized individuals with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2022;205(4):412–20. 10.1164/rccm.202103-0583OC
15 Bhavnani D, Lilley T, Rathouz PJ, Beaudenon-Huibregtse S, Davis MF, McCormack MC, et al. Indoor allergen exposure and its association to upper respiratory infections and pulmonary outcomes among children with asthma. J Allergy Clin Immunol. 2024;154(6):1434–441. 10.1016/j.jaci.2024.08.006
16 Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:71. 10.1136/bmj.n71
17 Peters MDJ, Godfrey C, McInerney P, Munn Z, Tricco AC, Khalil H. Scoping reviews. In: Aromataris E, Lockwood C, Porritt K, Pilla B, Jordan Z, editors. JBI Manual for Evidence Synthesis. JBI;2024. 10.46658/JBIMES-24-09
18 Dharmage S, Bailey M, Raven J, Mitakakis T, Guest D, Cheng A, et al. A reliable and valid home visit report for studies of asthma in young adults. Indoor Air. 1999;9(3):188–92. 10.1111/j.1600-0668.1999.t01-1-00005.x
19 Gehring U, Triche E, van Strien RT, Belanger K, Holford T, Gold DR, et al. Prediction of residential pet and cockroach allergen levels using questionnaire information. Environ Health Perspect. 2004;112(8):834–39. 10.1289/ehp.6685
20 de Souza B, Ferreira MA, Kalil J, Giavina-Bianchi P, Agondi RC. Development, validation and application of a questionnaire to qualify the indoor environmental exposure of patients with respiratory allergy. J Asthma. 2022;60(6):1191–201. 10.1080/02770903.2022.2138432
21 Punyadasa D, Adderley NJ, Rudge G, Nagakumar P, Haroon S. Self-reported questionnaires to assess indoor home environmental exposures in asthma patients: a scoping review. BMC Public Health. 2024;24:2915. 10.1186/s12889-024-20418-8
22 Robertson NM, Qui A, Raju S, McCormack MC, Koehler K. Cleaning indoor air-what works for respiratory health: an updated literature review and recommendations. J Allergy Clin Immunol. 2024;154(4):847–60. 10.1016/j.jaci.2024.08.011
23 Radbel J, Rebuli ME, Kipen H, Brigham E. Indoor air pollution and airway health. J Allergy Clin Immunol. 2024;154(4): 835–46. 10.1016/j.jaci.2024.08.013
24 Solarz K, Obuchowicz A, Asman M, Nowak W, Witecka J, Pietrzak J, et al. Abundance of domestic mites in dwellings of children and adolescents with asthma in relation to environmental factors and allergy symptoms. Sci Rep. 2021;11:18453. 10.1038/s41598-021-97936-7
25 Salo PM, Wilkerson J, Rose KM, Cohn RD, Calatroni A, Mitchell HE, et al. Bedroom allergen exposures in US households. J Allergy Clin Immunol. 2018;141(5):1870–1879. 10.1016/j.jaci.2017.08.033
26 Sabo A, Kuan G, Sarimah A, Kuay HS, Kueh YC. Psychometric properties of the newly developed self-report environmental determinants of health questionnaire (EDH-Q): development and validation. BMC Psychol. 2024;12:438. 10.1186/s40359-024-01782-x
27 Souza AC, Alexandre NMC, Guirardello EB. Psychometric properties in instruments evaluation of reliability and validity. Epidemiol Serv Saude. 2017;26(3):649–59. 10.5123/S1679-49742017000300022