
Download

REVIEW ARTICLE
Application of FeNO in the diagnostic and therapeutic algorithm of pediatric asthma: From chronic cough and wheeze to personalized management
Peter Kunča,b*, Jaroslav Fábrya, Peter Ferenca, Martina Neuschlováb, Renata Péčováb
aClinic of Pediatric Respiratory Diseases and Tuberculosis, Jessenius Faculty of Medicine in Martin (JFM CU), National Institute of Pediatric Tuberculosis and Respiratory Diseases, Comenius University in Bratislava, Dolny Smokovec, Slovak Republic
bJessenius Faculty of Medicine in Martin (JFM CU), Department of Pathological Physiology JFM CU, Comenius University in Bratislava, Slovak Republic
Abstract
Bronchial asthma is the most common chronic respiratory disease in children. Treatment approaches should aim to achieve disease control, reduce limiting symptoms, and improve quality of life. The routine management of patients with asthma relies on the assessment of symptoms (including persistent cough and wheezing) and spirometry results However, these strategies do not consider the level of airway inflammation, which is a fundamental pathognomonic feature of the disease. The use of biomarkers is increasing in an effort to better understand individual asthma pathways (endotyping), offering the potential for personalized treatment with innovative biologics. Elevated levels of fractional exhaled nitric oxide (FeNO) are an indirect marker of T2 airway inflammation. FeNO is one of the few biomarkers that has been implemented in routine clinical practice because of its undeniable advantages, such as accessibility, noninvasiveness, simple implementation, and cost-effectiveness. However, the current scientific evidence in children is insufficient to recommend its universal use in the diagnosis and treatment of all patients. Considering its known limitations, FeNO can enhance therapeutic processes, particularly in children with severe asthma. High FeNO levels predict a good therapeutic response to corticosteroids and selected biologics (e.g., omalizumab and dupilumab) and indicate an increased risk of exacerbation. Similarly, measuring FeNO levels in children with recurrent wheezing can help determine the risk of future asthma development. Various factors contributing to FeNO value variability must be considered when interpreting the results. The lack of robust clinical studies is reflected in inconsistent guidelines from professional societies regarding the use of FeNO in managing childhood asthma. This review aims to evaluate the advantages, disadvantages, and potential applications of FeNO measurements in light of new findings in the field.
Key words: asthma, biomarkers, children, exhaled nitric oxide, T2-high inflammation
*Corresponding authors: Renata Péčová, Jessenius Faculty of Medicine in Martin (JFM CU), Department of Pathological Physiology JFM CU, Comenius University in Bratislava, Slovak Republic. Email address: [email protected]
Received 1 October 2025; Accepted 1 January 2026; Available online 1 May 2026
Copyright: Kunč P, et al.
This open access article is licensed under Creative Commons Attribution 4.0 International (CC BY 4.0). http://creativecommons.org/licenses/by/4.0/
Introduction
Bronchial asthma is the most common chronic respiratory disease in children. Its prevalence is steadily increasing, leading to a significant economic impact on diagnosis and treatment, particularly in developed countries. According to an epidemiological analysis by the U.S. Centers for Disease Control and Prevention, the prevalence of asthma in the United States in 2017 was 7.9%, with a higher rate in children (8.4%) than in adults (7.7%).1
The primary hallmark of asthma is chronic lower airway inflammation associated with reversible bronchial hyperresponsiveness and structural changes in the tracheobronchial system. Recurrent bronchial obstruction underlies various clinical symptoms, including patient-reported dyspnea, wheezing, chest tightness, limited physical activity, and persistent cough. However, asthma is a heterogeneous clinical syndrome, particularly when comparing pediatric and adult populations. Childhood asthma is predominantly driven by a T2-high inflammatory endotype, unlike the more varied phenotypes observed in adults. This fundamental difference underscores the need for diagnostic tools that can accurately identify specific inflammatory pathways in children.2
Consequently, significant effort has been dedicated to understanding its diverse pathophysiological processes to identify different endotypes and phenotypes of the disease. Asthma treatment focuses on monitoring disease activity and severity while tailoring therapy to specific endotypes and phenotypes. However, spirometry parameters and reported symptoms may not directly quantify the severity of bronchial inflammation or fully predict the therapeutic response.
Diagnosing asthma, particularly in preschool-aged children, is a significant clinical challenge. The diagnostic process often relies on reported symptoms, such as frequent coughing or wheezing. However, these symptoms are non-specific and common in this age group, often representing transient conditions that resolve with age. This reliance on non-specific symptoms can lead to diagnostic uncertainty and the potential for both over- and underdiagnosis.3 Furthermore, the diagnostic approach is complicated by the inability of young children to reliably perform objective lung function tests, such as spirometry. Standard diagnostic methods (questionnaires, peak expiratory flow measurement, and spirometry) not only face feasibility issues in young children but also fail to assess the underlying airway inflammation, which is the principal therapeutic target.4 This discrepancy between symptoms, lung function, and the actual level of inflammation highlights a critical gap in the management of pediatric asthma in clinical practice.
Frequent coughing, recurrent virus-induced obstructive bronchitis, and wheezing are common in this age group; however, these are often transient conditions that resolve with age and appropriate management. Statistically, approximately 30% of children under six years of age experience at least one episode of wheezing within six months.5 Bronchial obstruction is a symptom, not a disease, and can be triggered by various factors, including infectious agents and environmental influences. Therefore, diagnosing asthma solely based on reported symptoms without objective verification may lead to overdiagnosis. Similarly, managing an asthmatic patient based only on symptom control may not be appropriate or successful in the long term, as symptom control does not always reflect the risk of future exacerbations.6 In clinical practice, discrepancies between parents’ subjective interpretation of symptoms and the child’s actual clinical presentation also pose challenges.
Beyond the cardinal symptoms, asthma imposes a substantial burden on the health-related quality of life of affected children, impacting physical, emotional, social, and school functioning. This burden is comparable, and in some domains even greater, than that reported for other major chronic childhood diseases such as type 1 diabetes, epilepsy, or juvenile idiopathic arthritis.7,8 Frequent school absenteeism, limitation of physical and social activities, sleep disturbances, and heightened anxiety contribute to a significant psychosocial impact on both the child and their family, underscoring the clinical urgency for precise diagnostic and effective management strategies.9,10
To fully comprehend and correctly interpret the clinical utility of FeNO in children, it is imperative to first elucidate the fundamental pathophysiological mechanisms of T2 inflammation that govern NO production. This narrative review, therefore, will first concisely summarize the key inflammatory pathways and subsequently provide a detailed, systematic overview of the evidence for the diagnostic and therapeutic application of FeNO in pediatric practice, culminating in a proposed clinical algorithm.
Methodology
This article is structured as an expert narrative review to bridge the gap between complex pathophysiology and clinical practice. To provide a comprehensive synthesis, we conducted a literature search using PubMed, Scopus, and Sciendo databases for articles published up to May 2025. The search strategy included the following keywords and their combinations: “fractional exhaled nitric oxide,” “FeNO,” “pediatric asthma,” “children,” “biomarkers,” “T2 inflammation,” and “biologics.” The study selection process is detailed in the flowchart (Figure 1). The selection process prioritized clinical trials, meta-analyses, systematic reviews, and guidelines from professional societies published in English. Preference was given to studies from the last 15 years to ensure the inclusion of the most current data; however, seminal older papers that were foundational to the topic were also included. Case reports, editorials, and studies focused exclusively on adult populations were excluded unless they provided essential context for asthma in children. Ultimately, 80 sources were selected for this review.
Figure 1 Flow chart of the literature selection process, Reasons for exclusion included: adult-only population (n=9), wrong publication type (n=4).
Clinically applicable biomarkers of asthma
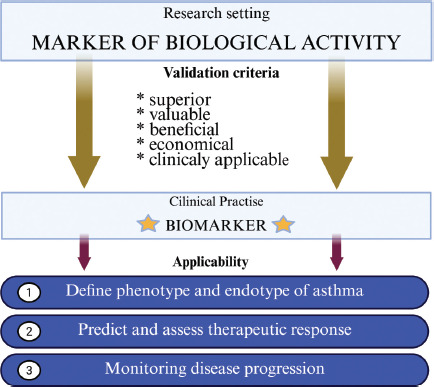
The identification of suitable noninvasive, clinically relevant, and cost-effective biomarkers is a key research goal for many diseases, including asthma. A valid, clinically applicable biomarker should be an additive tool for assessing therapeutic response, monitoring disease progression, and predicting the risk of future exacerbations. Another important function is distinguishing between individuals with the disease and healthy individuals. According to the “SAVED” model, an ideal biomarker should be “superior” (significantly helpful in practice), “valuable” (ability to modulate therapy), “cost-effective” (financially efficient), and clinically “applicable” (technological feasibility of the assay)11 (Figure 2). Despite considerable research into new potential biomarkers, only the measurement of fractional exhaled nitric oxide (FeNO) and eosinophil counts has been widely implemented in routine clinical practice.
Figure 2 Biomarker validation parameters, adapted from Hollnader et. al.11; created in Biorender.com.
Bronchial asthma and eosinophilic inflammation
The T2-high endotype, characterized by eosinophilic inflammation driven by Th2 lymphocytes and type 2 innate lymphoid cells (ILC2s), is predominant in childhood asthma. This endotype is characterized by inflammation, with a predominance of eosinophils in allergic or nonallergic terrain. This indicates that sensitization to inhalant allergens is not always present in pediatric patients. Considering this, laboratory sensitization to inhalant allergens does not have to be demonstrated in a proportion of pediatric patients. Damage to the airway epithelium by exogenous factors (allergens, viruses, and pollutants) leads to a loss of the functional and structural integrity of the bronchial epithelial barrier. Activation of innate and adaptive immune mechanisms results in the production of epithelial cytokines called alarmins (IL-25, IL-33, and thymic stromal lymphopoietin). Among these, TSLP is considered a key initiator of the T2 inflammatory cascade and is released by epithelial cells in response to various triggers.12 These alarmins directly activate Th2 and ILC2 cells to produce a characteristic cytokine spectrum (IL-4, IL-5, and IL-13) with pleiotropic functions.13 This cascade leads to characteristic functional and anatomical changes in the bronchi, such as goblet cell hyperplasia, smooth muscle hypertrophy, neovascularization, mucosal tissue fibrosis, and bronchial hyperresponsiveness.
Eosinophils are essential components of this inflammatory response. Furthermore, synthesized pro-inflammatory factors promote bronchial smooth muscle contractility and inhibit relaxation.14 IL-5, produced by immunocompetent cells, is crucial for the growth, maturation, and migration of pro-inflammatory eosinophils to the site of inflammation.15 Inflammation-activated epithelial cells also synthesize chemokines called eotaxins (e.g., CCL11 and CCL24). These eotaxins act as potent chemoattractants, binding to specific receptors on the eosinophil surface (e.g., CCR3) and triggering signaling pathways that result in their migration to the site of inflammation.16
Patients with the T2 endotype often show a good therapeutic response to inhaled corticosteroids (ICS) and a favorable response to bronchodilator therapy with beta-adrenergic receptor agonists. They also respond well to monoclonal antibodies that block T2 inflammatory cytokines. Elevated total IgE serves as a marker of atopy, supporting the diagnosis, but lacks specificity for T2-driven airway inflammation compared to FeNO or blood eosinophils.17 Typically, asthma endotyping focuses on eosinophil counts in the peripheral blood, induced sputum, or bronchoalveolar lavage fluid. However, collecting these biological materials from the pediatric population has significant limitations. Induced sputum examination is performed only in exceptional cases, as it requires active cooperation (problematic in young children) and inhalation of a hypertonic solution (risk of bronchospasms). Bronchoalveolar lavage requires invasive flexible bronchoscopy under general anesthesia, making it suitable only for severe and complex diagnostic cases. Although peripheral blood eosinophil counts are widely available, they do not always correlate with tissue eosinophil counts.18
A confirmed correlation between exhaled NO values and the number of eosinophils in bronchial mucosa histological samples has been demonstrated in children with difficult-to-treat asthma after treatment with systemic corticosteroids, favoring FeNO as a reliable marker.19 FeNO and eosinophils are both closely associated with T2-type inflammation, but their production is regulated by different inflammatory cascades (IL-5 for eosinophils vs. IL-13 for FeNO). Therefore, it is important to define their specific roles as independent, yet complementary, biomarkers for a holistic understanding of the disease.
Biology of nitric oxide
Nitric oxide (NO) is an inorganic chemical that is highly reactive in air and forms other nitrogen oxides. While it is known as an environmental pollutant, it serves as an important signaling molecule with various biological functions. NO acts as an intracellular messenger involved in the regulation of numerous processes in the endothelium, epithelium, and bronchial smooth muscle. Due to its functional importance, it is particularly prominent in the cardiovascular and respiratory systems of the body. The activity and production of NO are also influenced by the balance between pro-oxidant and antioxidant factors. All humans exhale NO. In a healthy population, approximately 40–45% of exhaled NO originates from the lower respiratory tract, with the remainder produced by epithelial cells of the upper respiratory tract.20 Unlike other mediators, it can diffuse freely across cell membranes into the airway lumen, which is a key feature that allows its measurement in exhaled air.
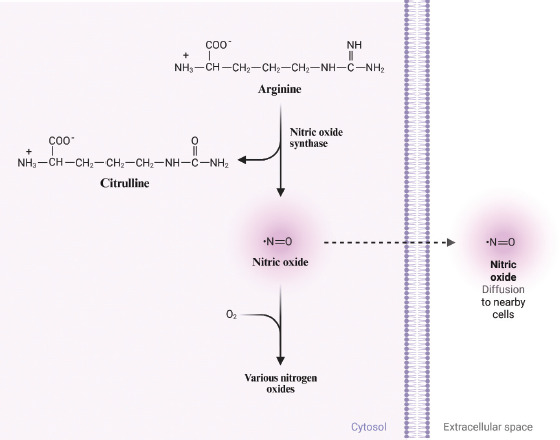
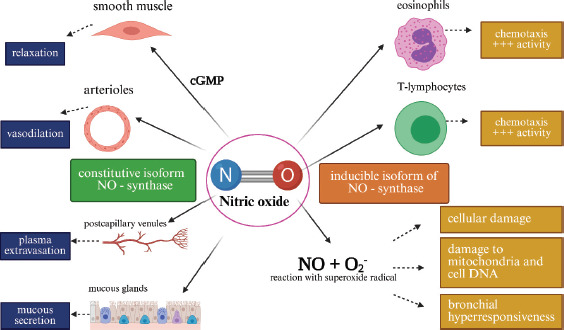
FeNO is produced in the airways by inflammatory cells through the oxidation of the amino acid L-arginine to form L-citrulline. This reaction is mediated by the NADPH-dependent inducible isoform of nitric oxide synthase (iNOS or NOS2)21 (Figure 3). NOS is expressed in three isoforms in humans. The activity of iNOS is upregulated by pro-inflammatory cytokines (IFN-γ, IL-1β), viruses, bacteria, allergens, and environmental pollutants; however, it is also constitutively maintained at a basal level by airway epithelial cells. Constitutive isoforms (nNOS or NOS1 and eNOS or NOS3) are produced by various pulmonary cells. NOS1, secreted by nonadrenergic, noncholinergic nerve endings, produces NO with myorelaxant effects on bronchial smooth muscle and vessel walls. NO, synthesized by NOS3 predominantly in the alveolar epithelium, primarily regulates the kinetics of airway cilia.22 The activity of constitutive isoforms is not affected by corticosteroids, whereas corticosteroids can suppress iNOS activity.21 Furthermore, IL-13, a central cytokine in T2 inflammation, is believed to increase the gene expression and transcription of mediators that support NOS2 production.23 The dual effects of NO on the airways are shown in Figure 4.
Figure 3 Schematic illustration of NO synthesis, created with Biorender.com.
Figure 4 Dual effect of NO in the pathophysiology of asthma, adapted from Song et. al. (52); created with Biorender.com, cGMP: Cyclic guanosine monophosphate
Measurement of exhaled NO
Elevated FeNO levels in children with asthma have been documented since 1997, particularly during disease exacerbations. These levels have been shown to significantly decrease following corticosteroid treatment.24,25 The measurement of FeNO has been standardized for clinical use by the American Thoracic Society/European Respiratory Society (ATS/ERS) guidelines.
The key advantages of this methodology include its noninvasive nature, repeatability, reproducibility, and ease of use. Its applicability in preschool-aged children is of significant clinical value. With modern devices employing electrochemical analysis, a success rate of approximately 70% can be achieved in children under five years of age.5 However, it is important to note that the standardized online single-breath method is often not feasible in preschool-aged children. Therefore, alternative techniques have been developed, such as the offline tidal breathing measurement method, which, although simpler, carries the risk of sample contamination from the nasal cavities and lacks flow rate control, which significantly influences FeNO values.
The measurement procedure is as follows: Following a full inhalation (to total lung capacity), the child exhales against low resistance (5–20 cm H2O), which ensures velopharyngeal closure to prevent contamination from nasal NO. During this exhalation, a constant expiratory flow rate of approximately 50 ml/s must be maintained for at least 6 s in children over 12 years old or 4 s in those younger than 12 years old. To encourage children to maintain the required expiratory duration, devices often use interactive and gamified displays. The results are expressed in parts per billion (ppb). Modern FeNO analyzers are typically compact, portable, and affordable. They facilitate easy, repeatable, and reliable measurements, yielding data that are suitable for clinical interpretation. This repeatability is particularly crucial, as it enables clinicians to monitor changes in FeNO levels over time, providing a valuable tool for assessing airway inflammation and the level of asthma control.
However, the practical application, especially in younger children, is not as straightforward as the standardized procedure suggests. Achieving reliable measurements in preschool-aged children requires considerable patience from both the child and the clinician. Young children often struggle to maintain the constant expiratory flow required, leading to the need for repeated attempts.26–28 It is crucial to emphasize that the success rate of measurements in children aged 3–5 years reported in studies ranges from approximately 50% to 80%, even under ideal conditions, and necessitates trained personnel.29–32 To mitigate these challenges, manufacturers have incorporated gamified visual feedback into the device software, such as animations of blowing out a candle or inflating a balloon, which can significantly improve a child’s cooperation and the success rate of the measurement.33,34
Cost-effectiveness and accessibility
Despite the clinical utility of FeNO, its widespread adoption in routine pediatric practice faces a significant and multifaceted barrier: cost and accessibility. This issue can be divided into several key components that collectively limit its use, particularly outside of specialized academic centers.
Firstly, the initial capital expenditure for a FeNO analysis device can be substantial for primary care offices or smaller clinics.35 This upfront investment is often a primary deterrent for healthcare providers operating under tight budgets. Secondly, beyond the device itself, there are ongoing operational costs associated with single-use sensors and disposable mouthpieces, which add a recurring expense for each test performed.
These direct financial outlays are compounded by inconsistent reimbursement policies from both public and private insurers. As highlighted in a recent Italian consensus, the lack of consistent inclusion of FeNO testing among exempt or fully reimbursed services for asthma patients represents a major barrier to equitable access.36 This situation is mirrored in many other healthcare systems, including the US, where payment for FeNO testing is often not guaranteed for all indications. This financial uncertainty discourages its integration into primary care and reinforces its status as a specialized tool, rather than a routine component of asthma management.37–39 Furthermore, it is pertinent to note that reimbursement policies and accessibility vary dramatically not only between the US and Europe but also among individual European nations, thereby limiting its universal implementation according to standardized guidelines.40
However, the debate on cost-effectiveness is nuanced and cannot be judged solely on the per-test cost. Several pharmacoeconomic analyses from various countries, including Italy, Sweden, the UK, and the US, suggest that the strategic use of FeNO could be cost-effective in the long run.39,41 The rationale is that a more precise, biomarker-guided approach can lead to significant downstream savings. For instance, by accurately identifying patients who will respond to inhaled corticosteroids or by guiding the appropriate use of expensive biologic therapies, FeNO has the potential to prevent costly exacerbations, emergency room visits, and hospitalizations. One Italian study estimated that more extensive use of FeNO could lead to an annual reduction in direct medical costs of up to 13% per patient.42 Nevertheless, for now, these economic considerations remain a major deterrent to its universal accessibility in pediatric asthma care.43
Variability of FeNO
FeNO levels are influenced by various determinants and should be interpreted in the context of the clinical history and presentation. Factors that can impact measured values include atopy, height, age, sex, race, respiratory tract infections, consumption of nitrates, caffeine, alcohol, and active or passive smoking (Table 1).22 Paradoxically, some conditions can lead to lower FeNO values; for instance, active or passive smoking and acute bronchoconstriction are known to decrease exhaled NO levels. Furthermore, recent meta-analyses of randomized controlled trials have not demonstrated that vitamin D supplementation, despite its known immunomodulatory effects, significantly influences FeNO values, which further refines our understanding of the factors modulating this key biomarker.44
Table 1 Factors Influencing FeNO Levels in Children.
| Category | Factors that increase FeNO | Factors that decrease FeNO | Pediatric considerations |
|---|---|---|---|
| Physiological22 | Male sex, increasing age and height (up to puberty), ethnicity (e.g., African American) | - | Values must be interpreted in the context of age- and height-specific reference ranges. |
| Co-morbidities76 | Allergic rhinitis, atopic dermatitis, eosinophilic bronchitis | Acute bronchoconstriction | Atopy is a major confounder and should always be assessed. |
| Lifestyle/Environmental45 | Nitrate-rich diet, intense physical exercise | Active and passive smoking, alcohol | Passive smoking is a key factor in the pediatric population (adolescents) |
| Infections47 | Acute viral respiratory infections | - | FeNO measurement should be postponed during acute infections. |
| Medications49 | Some antihistamines | Inhaled and systemic corticosteroids | Response to ICS is a key clinicalutility of FeNO measurement. |
Obesity is a significant factor and a growing global health problem, often associated with poor asthma control. Dysregulation of metabolic and neuroendocrine processes in adipose tissue enhances systemic inflammation. Surprisingly, despite significant sputum eosinophilia often found in obese patients, lower FeNO values have been reported.45
Exhaled NO also exhibits a diurnal rhythm, and studies have shown that morning measurements are significantly higher than those taken at night.46 While systemic and inhaled corticosteroids decrease FeNO levels, some antihistamines may paradoxically increase them.47 Naturally, coexisting T2-related conditions, such as atopic dermatitis, allergic rhinitis, and eosinophilic bronchitis, also contribute to elevated exhaled NO levels. Furthermore, exercise is another important consideration, as clinical studies have demonstrated that intense physical activity can result in higher FeNO levels than in less active children and adolescents.48
Age, height, and sex are critical physiological determinants in pediatric patients. FeNO values showed a linear increase with age and height in girls aged 6–14 years and boys aged 6–16 years. Subsequently, both sexes reach a plateau in adolescence, which persists into adulthood.49,50 Ethnicity and race also predict different basal FeNO levels. For example, studies in the US have found that Hispanic and African American children tend to have higher mean FeNO levels than their Caucasian counterparts.51
Given the many determinants of FeNO variability, it is crucial to interpret the results in correlation with the patient’s complete clinical picture. Some studies have suggested the use of FeNO measurements to aid in the detection of cough-variant asthma and eosinophilic bronchitis in adults with chronic cough.52 The authors of this article previously investigated the possible association between FeNO and cough reflex sensitivity in childhood asthma and found no correlation between elevated FeNO values and increased cough reactivity in either asthmatic or healthy children.53 Conversely, concerning post-infectious cough, FeNO measurement has not proven to be a useful biomarker for monitoring patients after COVID-19 infection, as FeNO levels were not significantly elevated compared to healthy controls. This suggests that persistent cough in the post-COVID-19 syndrome may not be associated with underlying T2 eosinophilic airway inflammation.54
Application of FeNO in clinical practice
FeNO values indirectly reflect the degree of eosinophilic airway inflammation in the lungs. In the presence of eosinophilic inflammation (which correlates with eosinophil counts in blood and bronchoalveolar lavage fluid, serum eosinophil cationic protein, and total IgE), iNOS is activated in the airway epithelium by proinflammatory cytokines, leading to increased NO production. Thus, FeNO can be considered an indirect marker of IL-13 activity in T2-high asthma patients. A summary of the evidence for the clinical application of FeNO based on the reviewed literature is presented in Table 2.
Table 2 Summary of Evidence for the Clinical Application of FeNO in Pediatric Asthma, sources: (22); (76); (45); (47); (49).
| Clinical application | Key Findings/consensus | Strength of evidence | Relevant studies(examples) |
|---|---|---|---|
| Asthma Diagnosis | High FeNO supports diagnosis of T2-inflammatory asthma, especially in atopic children. High specificity, lower sensitivity. | Moderate-High | (69); (70) |
| Prediction of Future Asthma | Elevated FeNO in preschoolers with wheeze is a predictor of later asthma development. | Moderate | (58); (59) |
| Guiding ICS Therapy | High FeNO predicts good response to ICS. FeNO-guided therapy can reduce exacerbations but may lead to higher ICS doses. | High | (19); (61) |
| Predicting Response to Biologics | High FeNO is a strong predictor of good response to anti-IL-4Rα (Dupilumab) and anti-TSLP (Tezepelumab). Synergistic with eosinophils for anti-IL-5 (Mepolizumab). | High | (77); (79) |
Note: The Strength of Evidence is graded based on the hierarchy of evidence, with the highest weight given to systematic reviews and meta-analyses of randomized controlled trials (RCTs), followed by individual RCTs and prospective cohort studies.
The diagnostic utility of FeNO in identifying patients with eosinophilic asthma who are likely to benefit from ICS has been confirmed in systematic reviews.13 Conversely, because elevated FeNO values also occur in other atopic diseases, some authors have suggested that low FeNO values are better at predicting a non-T2 endotype than high values are at confirming a T2 endotype.55 Studies in preschool children have shown that FeNO can be a useful tool for objectively distinguishing between different wheezing phenotypes (e.g., persistent vs. transient wheeze) and assessing the risk of later asthma development or impaired lung growth. Although data on its added value compared to clinical parameters (such as the Asthma Predictive Index) are sometimes conflicting, some studies have confirmed that FeNO has an additive predictive value beyond clinical history and the presence of specific IgE antibodies56,57 (Table 3).
Table 3 Selected studies on the diagnostic and predictive value of FeNO in children.
| Author(s) & year | Study type | Participants (n) | Age group | Key findings |
|---|---|---|---|---|
| Caudri et al. (2010); (58) | Prospective birth cohort study | 308 (for FeNO) | Measured at 4 years, follow-up to 8 years | FeNO measured at age 4 in symptomatic children improved the prediction of asthma symptoms at age 8, independent of clinical history. |
| Di Cara et al. (2015); (59) | Prospective study | 88 | 6-14 years | In children with allergic rhinitis, a baseline FeNO > 35 ppb was associated with a significantly higherrisk of developing asthma over a 5-year follow-up. |
| Oh et al. (2013); (56) | Cross-sectional study | 372 | 4 and 6 years | Children with persistent wheeze had significantly higher FeNO levels than those with transient wheeze or no wheeze, suggesting FeNO can help differentiate phenotypes. |
| Karrasch et al. (2017); (69) | Systematic review & meta-analysis | 4,518 (from 26 studies) | Children & Adults | FeNO demonstrated fair diagnostic accuracy, with higher specificity (0.82) than sensitivity (0.65), indicating a stronger potential for confirming (“ruling in”) asthma. |
| Pijnenburg (2019); (70) | Review | N/A | Preschool & School-aged children | High FeNO in preschoolers predicts later asthma and impaired lung growth. In symptomatic, atopic school children, it has diagnostic value, primarily for “ruling in” asthma. |
Elevated levels of this biomarker in high-risk preschoolers with recurrent broncho-obstructive attacks strongly correlate with the risk of developing and maintaining asthma later in life.58 This test also has significant diagnostic implications for school-aged children with atopic asthma. Children with FeNO in the highest quartile in population-based studies were more than twice as likely to receive a new diagnosis of asthma at an older age.59,60 Furthermore, in children with allergic rhinitis, a baseline FeNO value > 35 ppb has been associated with a higher risk of future asthma development and slower lung function growth (FEV1 and FVC) over a 5-year follow-up period.59 A recent meta-analysis demonstrated that asthma management guided by FeNO led to a reduction in exacerbations and better ventilation parameters in the study cohort than in the control group, although the FeNO-guided group received higher average daily doses of ICS61 (Table 4). Nine randomised clinical trials including 1885 children have added FeNO to usual asthma care and found that exacerbations are reduced when care is guided by FeNO (OR for exacerbation compared to usual care 0.77, 95% CI 0.62–0.94).62 However, it is crucial to acknowledge the contrasting evidence from the recent large-scale RAACENO trial, the largest of its kind in children, which found no significant reduction in asthma exacerbation rates when FeNO was used to guide treatment compared to standard guideline-based care.63
Table 4 Selected studies on FeNO for guiding therapy and predicting corticosteroid response.
| Author(s) & year | Study type | Participants (n) | Age Group | Intervention | Key findings |
|---|---|---|---|---|---|
| Baraldi et al. (1997); (25) | Clinical trial | 16 | 6-13 years | 5 days of oral prednisone for acute asthma | Oral steroids led to a mean 46% decrease in FeNO levels, demonstrating a rapid response to anti-inflammatory treatment. |
| Payne et al. (2001); (19) | Clinical study | 31 | 6-17 years | 2 weeks of oral prednisolone in difficult-to-treat asthma | A significant correlation (r=0.54) wasfound between FeNO and eosinophil score from biopsies, confirming FeNO as a non-invasive marker of eosinophilic inflammation. |
| Wang et al. (2020)*; (61) | Systematic review & meta-analysis | 23 randomized controlled trials | Children | FeNO-guided vs. standard asthma management | FeNO-guided management led to a significant reduction in asthma exacerbations compared to standardcare, albeit at the expense of increased ICS use. |
| Dinh-Thi-Dieu etal. (2020); (68) | Randomized controlled trial | 224 | Mean age 10-11 years | FeNO-guided ICS titration vs. GINA guidelines alone | The FeNO-guided group had significantly lower daily ICS doses and treatment costs after 12 monthswithout compromising asthma control. |
| Fraser et al. (2023); (62) | Systematic review & meta-analysis | 1885 (from 9 RCTs) | Children | FeNO-guided vs. standard asthma management | FeNO-guided care is associated with reduced odds of exacerbation (OR 0.77, 95% CI 0.62-0.94). |
Elevated FeNO (>35 ppb) in children generally indicates eosinophilic inflammation and predicts a higher risk of relapse when reducing ICS therapy. Prospective clinical studies have associated elevated NO concentrations in exhaled air with an increased risk of recurrent transient wheezing in preschool-aged children. High values in toddlers with recurrent wheezing also predict a decline in spirometry parameters during school age.5 In contrast, a low value (<20 ppb) in symptomatic, corticosteroid-naïve pediatric patients is associated with a lower likelihood of eosinophilic inflammation and a poorer response to ICS treatment. Values between 20 and 35 ppb fall into a “grey zone” with unclear clinical interpretation.64 A reduction of at least 20% for values >50 ppb or a reduction of >10 ppb for values <50 ppb indicates a significant response to anti-inflammatory ICS therapy.65
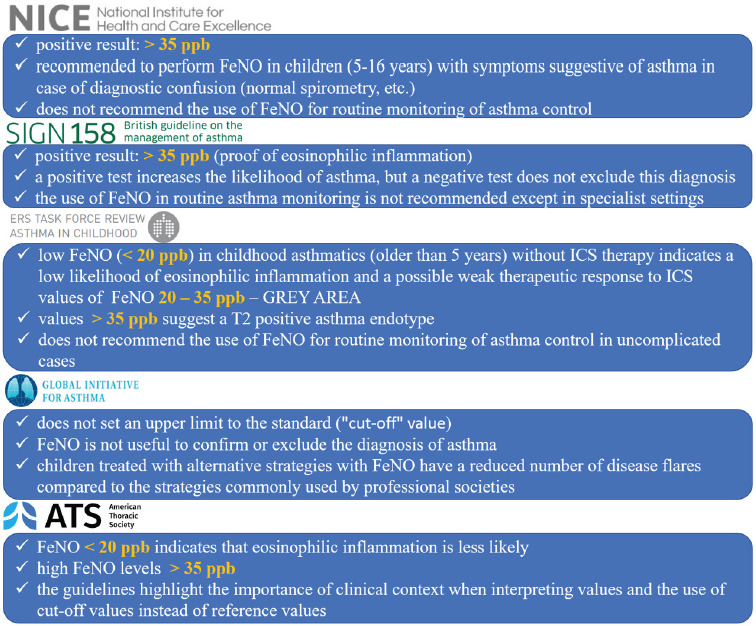
However, there is no consensus on the implementation of FeNO in routine clinical practice, and published guidelines often conflict with each other. These discrepancies can be explained by the limited number of studies in children compared to the adult population, making it difficult to adequately assess the strength of evidence. The main aspects of FeNO implementation in asthma management according to the selected professional societies are summarized in Figure 5. Furthermore, it is not clear what cut-off(s) of FeNO should be used to trigger a change in treatment, and after 30 years of intensive research, there is insufficient evidence to recommend FeNO for routine diagnosis and monitoring of asthma in children.62
Figure 5 Guidelines of societies and implementation of FeNO in children with asthma, source of data: https://www.nice.org.uk/, https://www.brit-thoracic.org.uk/, https://www.ersnet.org/, https://ginasthma.org/, https://www.thoracic.org/.
According to systematic reviews and meta-analyses, FeNO is not only a valuable diagnostic tool but also a biomarker for the efficacy of and adherence to anti-inflammatory treatment under certain circumstances.66 Despite these promising results, the 2022 Global Initiative for Asthma (GINA) guidelines concluded that FeNO testing is not generally helpful for confirming or excluding an asthma diagnosis or for guiding therapeutic management in the general population. However, the same GINA report recommends that treatment strategies adjusted based on FeNO changes can reduce exacerbations in children compared to standard approaches.67 In contrast to the general GINA recommendations, one study confirmed the benefit of an FeNO-guided approach in combination with GINA guidelines for ICS titration, showing it to be a useful tool for reducing daily ICS doses and the associated economic burden.68
Available data from meta-analyses provide evidence of the diagnostic significance of FeNO in corticosteroid-naïve patients with asthma. The test’s specificity (82%, 95% CI: 0.76–0.86) is higher than its sensitivity (65%, 95% CI: 0.58-0.72). This suggests that FeNO testing is more appropriate for confirming the diagnosis than for ruling out disease. While increased values correlate with a greater likelihood of a positive diagnosis, low concentrations of exhaled NO do not exclude asthma.69 Its diagnostic value is particularly high in symptomatic and atopic school-aged children, where it is especially helpful for confirming an asthma diagnosis (ruling in asthma).70
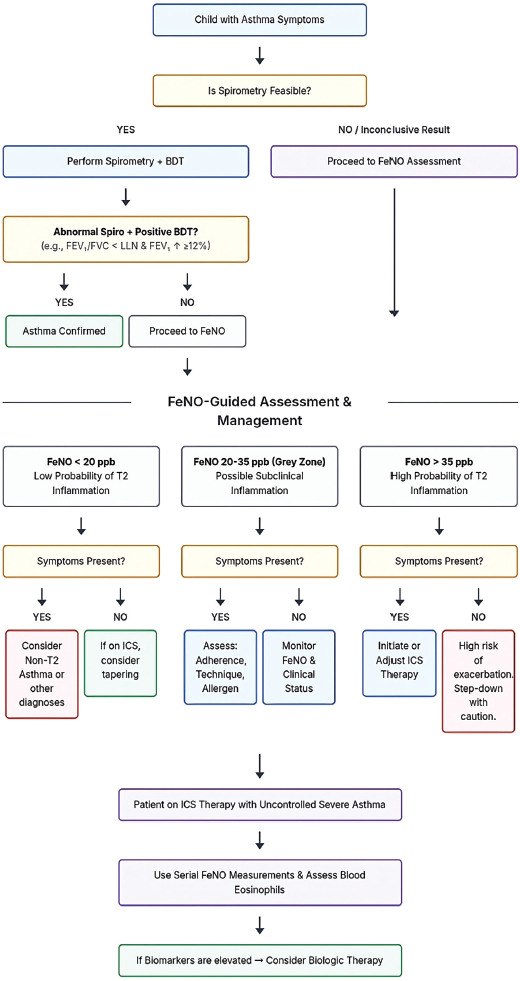
The proposed clinical algorithm (Figure 6) synthesizes these findings into a practical decision-making tool. The rationale for the cut-off values is derived from international guidelines (e.g., ATS/ERS), wherein a value <20 ppb indicates a low probability of significant eosinophilic inflammation and, consequently, a reduced likelihood of response to inhaled corticosteroids (ICS). Conversely, a value >35 ppb in children is strongly suggestive of underlying T2 inflammation and predictive of a favorable response to ICS. This principle is applied within the algorithm for both diagnostic purposes (in symptomatic, ICS-naïve patients) and therapeutic management (e.g., when considering ICS de-escalation). For patients falling within the ‘grey zone’ (20–35 ppb), the algorithm underscores the necessity of integrating the complete clinical context, including atopic status and prior treatment response, as the FeNO value alone possesses limited discriminatory power in this range.
Figure 6 Clinical Algorithm for Pediatric Asthma: Integrating FeNO Measurement. (Notes: BDT, Bronchodilator Test; FeNO, Fractional exhaled Nitric Oxide; FEV1, Forced Expiratory Volume in 1 second; FVC, Forced Vital Capacity; ICS, Inhaled Corticosteroids; LLN, Lower Limit of Normal; ppb, parts per billion.)
FeNO and selection of biologics
Severe asthma that is refractory to conventional treatment is a serious health problem. Although pediatric asthma is often more treatable than adult asthma, severe cases do occur in children. Innovative biologics are available when disease control is not achieved with standard therapy. These drugs are licensed monoclonal antibodies that block the T2 inflammatory pathway by targeting associated cytokines and IgE antibodies. Selective biomarkers can help identify suitable responders; pivotal studies in this domain are summarized in Table 5.
Table 5 Role of FeNO in predicting response to biologic therapies.
| Biologic | Key study/analysis | Participants (n) | Age group | Key finding regarding FeNO |
|---|---|---|---|---|
| Omalizumab | Casale et al. (2019) (PROSPERO post-hoc); (72) | 822 | ≥12 years | Patients with baseline FeNO > 19.5 ppb had a significantly greater reduction in exacerbations (53% vs. 16%) compared to those with lower FeNO levels. |
| Mepolizumab | Shrimanker et al. (2019) (DREAM post-hoc); (75) | 606 | Adults | Showed greatest efficacy (62% exacerbation reduction) in patients with both high blood eosinophils (≥150/μL) and high FeNO (≥25 ppb). No significant effect was seen in patients with low eosinophils, regardless of FeNO level. |
| Dupilumab | Busse et al. (2021) (QUEST post-hoc analysis); (77). | 934 | Adults | Showed greatest efficacy (68% exacerbation reduction) in patients with high eosinophils and highFeNO. A significant reduction (39%) was also seen in patients with low eosinophils but high FeNO. |
| Tezepelumab | Menzies-Gow et al. (2021) (NAVIGATOR); (79) | 1,061 | ≥12 years | Significantly reduced exacerbations by 56% vs. placebo in a broad population. Further analyses showed patients with higher baseline FeNO levels experienced a greater reduction in exacerbations. |
Omalizumab, the first approved monoclonal antibody for asthma with over two decades of clinical use, is an IgE-blocking IgG1 antibody indicated for children aged 6 years and older.71 It prevents IgE from binding to its receptors on cell surfaces. The role of FeNO in selecting patients and predicting therapeutic responses remains unclear.23 A post-hoc analysis of pediatric patients (>12 years) showed that those with higher baseline FeNO levels (>19.5 ppb) had a more significant reduction in exacerbations after 48 weeks of omalizumab treatment (53% vs. 16%) than those with lower FeNO levels.72
Mepolizumab is an IgG1 monoclonal antibody targeting IL-5, the major cytokine involved in eosinophil migration, maturation, and activation. It is approved for children aged six years and older with severe eosinophilic asthma.71 Studies have not consistently supported the relevance of FeNO as a biomarker of therapeutic success with mepolizumab.73,74 This is likely because FeNO production is primarily driven by the IL-13 pathway, whereas mepolizumab targets the IL-5 pathway of eosinophil differentiation. Nevertheless, a post-hoc analysis of the DREAM trial showed that adult patients treated with mepolizumab who had both high FeNO (>25 ppb) and high blood eosinophils (≥300 cells/μL) experienced a more significant reduction in exacerbations than the group with low FeNO and high eosinophils (62% vs. 34%), suggesting a synergistic predictive value of these two biomarkers.75
Dupilumab blocks the α-subunit of the IL-4 receptor (IL-4Rα), which is a common co-receptor for both IL-4 and IL-13. This dual mechanism effectively inhibits the signaling of both key pro-inflammatory cytokines, leading to broad downregulation of T2 inflammation across different allergic disorders. It is indicated for patients aged six years and older with allergic or non-allergic eosinophilic asthma and FeNO >25 ppb, or for those dependent on oral corticosteroids, regardless of their blood eosinophil count.71,76 The role of FeNO as a predictor of a good therapeutic response was confirmed in the Liberty Asthma Quest trial. Participants aged 12 years and older with baseline FeNO values >25 ppb had a significantly reduced exacerbation rate (approximately 50%) compared to patients with FeNO <25 ppb.77 The study further demonstrated that a higher baseline FeNO value was associated with a more significant therapeutic response to dupilumab, even after adjusting for blood eosinophil levels, thereby confirming its role as an independent predictor. These findings strongly support the clinical recommendation that, prior to initiating treatment with biologics such as dupilumab, baseline serum eosinophils and FeNO should be measured to more accurately identify patients who will benefit most from the therapy. Furthermore, a consistent decrease from baseline FeNO values in patients receiving chronic anti-IL-4Rα treatment suggests its potential as a pharmacodynamic biomarker for dupilumab.78
Tezepelumab, recently approved for adolescents aged 12 years and older, targets a key alarmin positioned at the top of the inflammatory cascade that plays a pivotal role in the pathogenesis of T2-driven diseases such as asthma and chronic rhinosinusitis with nasal polyps.12,71 The European Medicines Agency (EMA) has approved it for adolescents (≥12 years) and adults with severe asthma, regardless of phenotype or biomarker status. In clinical trials, tezepelumab reduced eosinophil counts, FeNO, and IgE levels, suggesting its broad suppressive action on multiple inflammatory pathways. Similar to dupilumab, patients with higher baseline FeNO levels experience a significant reduction in disease flares.79 While innovative biologics are highly effective, it is important to consider their potential risks, which include an increased susceptibility to certain infections and, in rare cases, allergic or autoimmune reactions.80
Studies on biologics have mainly focused on the utility of FeNO in predicting therapeutic responses. However, few studies have assessed the significance of dynamic changes in FeNO during treatment. The prognostic relevance of these changes, particularly when considering switching biologics, could be a valuable subject for future studies.
Conclusions
Asthma is a complex, multifactorial disease, and like other allergic conditions, its prevalence in children is expected to continue to rise. In clinical practice, the diagnosis and management of pediatric asthma are predominantly based on symptom evaluation. This approach, however, has limitations and can lead to misdiagnosis. Therefore, methods that assess the functional status of the airways, including bronchial hyperresponsiveness, have an irreplaceable place in the diagnostic algorithm. Yet, these tests do not directly measure the severity of airway inflammation, the principal pathognomonic entity of asthma. It is precisely in this context that FeNO becomes a key tool, enabling the transition from symptomatic to personalized, endotype-driven management of pediatric asthma. This fulfils the concept of precision medicine, where treatment is not focused merely on suppressing symptoms but on influencing the underlying pathophysiological basis of the disease. While current evidence cautions against its routine use for general monitoring, its targeted application in specific clinical scenarios is invaluable. By objectively quantifying T2-driven inflammation, FeNO helps clinicians deconstruct the heterogeneity of childhood asthma, thereby guiding more rational therapeutic choices, from initiating corticosteroids to selecting specific biologics.
Based on the synthesized evidence presented, FeNO is a non-invasive, easy-to-implement, repeatable, and cost-effective biomarker that reflects the level of T2 inflammation in the bronchi, driven by IL-13 activity in the airway epithelium. It represents an additional tool to improve the diagnosis and follow-up of pediatric patients with asthma. As summarized in our evidence tables, FeNO does not replace standard methods but complements them meaningfully when appropriately indicated and interpreted, proving particularly beneficial in severe and complex cases. The relationship between decreasing FeNO values and the effects of inhaled and systemic corticosteroids suggests its role as a predictor of therapeutic response and an indirect measure of treatment adherence. Additionally, it may help stratify patients by future risk of exacerbation and decline in spirometry parameters. Recent findings have also highlighted the importance of FeNO in predicting and monitoring the response to selected biologics (omalizumab, dupilumab, tezepelumab).
Naturally, this biomarker has limitations. Its values are influenced by numerous endogenous and exogenous factors. Guidelines from professional societies for pediatric patients are not uniform and are often contradictory, a result of the lack of robust, large-scale studies comparable to those in adults. There is also a discrepancy in recommended reference values.
Furthermore, this review has several limitations that must be acknowledged. The primary limitation is its nature is its nature as a narrative, rather than a systematic, review. This means the literature search was not conducted following a strict methodology, such as PRISMA, and therefore the selection of studies could be influenced by the authors’ subjective approach. Secondly, our conclusions may be affected by publication bias, as studies reporting positive or statistically significant results are more likely to be published than those with negative or inconclusive findings. Finally, our review was restricted to literature published in the English language, which may have resulted in the omission of relevant research from other regions. We acknowledge that, due to these factors, the work is susceptible to selection bias, as rightly pointed out by the reviewer. The implementation of further high-quality, large-scale studies will be essential to better understand the role and targeted use of FeNO in children with asthma.
Future Perspective
In the next decade, the role of FeNO in pediatric asthma is poised to transition from a specialized biomarker to an integral component of personalized medicine, driven by technological and methodological advancements. We anticipate the results of large-scale, prospective international studies that will definitively clarify its utility in long-term management, focusing not only on preventing exacerbations but also on preserving future lung growth and function. A significant leap forward will likely involve the integration of FeNO measurements with other omics data, such as genomics and proteomics into advanced machine-learning algorithms. These digital tools could generate highly accurate, individualized risk profiles, predicting the ideal therapeutic pathway for each child and moving beyond the simple “T2-high” classification to identify more subtle inflammatory sub-endotypes. Furthermore, we foresee the development of more affordable, user-friendly FeNO devices connected to digital health platforms, enabling remote monitoring and facilitating its seamless integration into primary care. This evolution will ultimately solidify FeNO’s position not merely as a diagnostic aid, but as a cornerstone of a proactive, predictive, and truly personalized approach to managing childhood asthma.
Acknowledgements
This work was supported by the project of Ministry of Education, Research, Development and Youth of the Slovak Republic; VEGA 1/0024/23. The funder had no role in the design, data collection, data analysis, and reporting of this study.
Mandatory Disclosure on Use of Artificial Intelligence
The authors declare that no AI-assisted tools were used in the preparation of this manuscript. All references have been manually verified for accuracy and relevance.
Author Contributions
All authors contributed equally to this article
Conflict of Interest
The authors declare no conflict of interest.
REFERENCES
1 Stern J, Pier J, Litonjua AA. Asthma epidemiology and risk factors. Semin Immunopathol. 2020 Feb;42(1):5-15. 10.1007/s00281-020-00785-1
2 Licari A, Castagnoli R, Brambilla I, Marseglia A, Tosca MA, Marseglia GL, et al. Asthma Endotyping and Biomarkers in Childhood Asthma. Pediatr Allergy Immunol Pulmonol. 2018 June 1;31(2):44-55. 10.1089/ped.2018.0886
3 Bacharier LB, Guilbert TW. Diagnosis and management of early asthma in preschool-aged children. Journal of Allergy and Clinical Immunology. 2012 Aug 1;130(2):287-96. 10.1016/j.jaci.2012.04.025
4 Jat KR, Agarwal S. Lung Function Tests in Infants and Children. Indian J Pediatr. 2023 June 1;1-8. 10.1007/s12098-023-04588-8
5 Elenius V, Chawes B, Malmberg PL, Adamiec A, Ruszczyński M, Feleszko W, et al. Lung function testing and inflammation markers for wheezing preschool children: A systematic review for the EAACI Clinical Practice Recommendations on Diagnostics of Preschool Wheeze. Pediatric Allergy and Immunology. 2021;32(3):501-13. 10.1111/pai.13418
6 Wu AC, Tantisira K, Li L, Schuemann B, Weiss ST, Fuhlbrigge AL. Predictors of Symptoms Are Different From Predictors of Severe Exacerbations From Asthma in Children. Chest. 2011 July;140(1):100-7. 10.1378/chest.10-2794
7 Pande V, Thakur M. Emphasis on Quality of Life in Children and Adolescents With Bronchial Asthma. Cureus. 2024 Sept;16(9):e68762. 10.7759/cureus.68762
8 Bhagat D, Fagnano M, Halterman JS, Reznik M. Asthma Symptoms, Interactive Physical Play, and Socio-emotional and Academic Outcomes in Urban Children with Persistent Asthma. J Asthma. 2019 July;56(7):711-8. 10.1080/02770903.2018.1488978
9 Allen CW, Diamond-Myrsten S, Rollins LK. School Absenteeism in Children and Adolescents. Am Fam Physician. 2018 Dec 15;98(12):738-44.
10 Koinis-Mitchell D, Kopel SJ, Farrow ML, McQuaid EL, Nassau JH. Asthma and Academic Performance in Urban Children. Ann Allergy Asthma Immunol. 2019 May;122(5):471-7. 10.1016/j.anai.2019.02.030
11 Hollander Z, DeMarco ML, Sadatsafavi M, McManus BM, Ng RT, Sin DD. Biomarker Development in COPD: Moving From P Values to Products to Impact Patient Care. Chest. 2017 Feb;151(2):455-67. 10.1016/j.chest.2016.09.012
12 Moreno-Jiménez E, Morgado N, Gómez-García M, Sanz C, Gil-Melcón M, Isidoro-García M, et al. TSLP and TSLPR Expression Levels in Peripheral Blood as Potential Biomarkers in Patients with Chronic Rhinosinusitis with Nasal Polyps. International Journal of Molecular Sciences. 2025 Jan;26(3):1227. 10.3390/ijms26031227
13 Pavord ID, Beasley R, Agusti A, Anderson GP, Bel E, Brusselle G, et al. After asthma: redefining airways diseases. Lancet. 2018 27;391(10118):350-400. 10.1016/S0140-6736(17)30879-6
14 Farne HA, Wilson A, Powell C, Bax L, Milan SJ. Anti-IL5 therapies for asthma. Cochrane Database Syst Rev. 2017 Sept 21;9:CD010834. 10.1002/14651858.CD010834.pub3
15 Agache I, Strasser DS, Klenk A, Agache C, Farine H, Ciobanu C, et al. Serum IL-5 and IL-13 consistently serve as the best predictors for the blood eosinophilia phenotype in adult asthmatics. Allergy. 2016 Aug;71(8):1192-202. 10.1111/all.12906
16 Williams TJ. Eotaxin-1 (CCL11). Front Immunol. 2015;6:84. 10.3389/fimmu.2015.00084
17 Cazzola M, Ora J, Cavalli F, Rogliani P, Matera MG. Treatable Mechanisms in Asthma. Mol Diagn Ther. 2021;25(2):111-21. 10.1007/s40291-021-00514-w
18 Jesenak M, Zelieskova M, Babusikova E. Oxidative Stress and Bronchial Asthma in Children-Causes or Consequences? Front Pediatr. 2017;5:162. 10.3389/fped.2017.00162
19 Payne DN, Adcock IM, Wilson NM, Oates T, Scallan M, Bush A. Relationship between exhaled nitric oxide and mucosal eosinophilic inflammation in children with difficult asthma, after treatment with oral prednisolone. Am J Respir Crit Care Med. 2001 Oct 15;164(8 Pt 1):1376-81. 10.1164/ajrccm.164.8.2101145
20 Wang Z, Pianosi P, Keogh K, Zaiem F, Alsawas M, Alahdab F, et al. The Clinical Utility of Fractional Exhaled Nitric Oxide (FeNO) in Asthma Management [Internet]. Agency for Healthcare Research and Quality; 2017 [cited 2021 Mar 19]. Available from: https://effectivehealthcare.ahrq.gov/topics/asthma-nitric-oxide/research/
21 Hoyte FCL, Gross LM, Katial RK. Exhaled Nitric Oxide: An Update. Immunol Allergy Clin North Am. 2018 Nov;38(4):573-85. 10.1016/j.iac.2018.06.001
22 Rao DR, Phipatanakul W. An Overview of Fractional Exhaled Nitric Oxide and Children with Asthma. Expert Rev Clin Immunol. 2016 May;12(5):521-30. 10.1586/1744666X.2016.1141049
23 Loewenthal L, Menzies-Gow A. FeNO in Asthma. Semin Respir Crit Care Med. 2022 Oct;43(5):635-45. 10.1055/s-0042-1743290
24 Nelson BV, Sears S, Woods J, Ling CY, Hunt J, Clapper LM, et al. Expired nitric oxide as a marker for childhood asthma. J Pediatr. 1997 Mar;130(3):423-7. 10.1016/S0022-3476(97)70204-X
25 Baraldi E, Azzolin NM, Zanconato S, Dario C, Zacchello F. Corticosteroids decrease exhaled nitric oxide in children with acute asthma. J Pediatr. 1997 Sept;131(3):381-5. 10.1016/S0022-3476(97)80062-5
26 Nystad W, Samuelsen SO, Nafstad P, Edvardsen E, Stensrud T, Jaakkola JJK. Feasibility of measuring lung function in preschool children. Thorax. 2002 Dec;57(12):1021-7. 10.1136/thorax.57.12.1021
27 Fenu G, Calogero C, Lombardi E. Lung Function Tests in Preschool Children. Turk Thorac J. 2015 Oct;16(4):185-8. 10.5152/ttd.2015.5038
28 Gaffin JM, Shotola NL, Martin TR, Phipatanakul W. Clinically Useful Spirometry in Preschool-Aged Children: Evaluation of the 2007 American Thoracic Society Guidelines. J Asthma. 2010 Sept;47(7):762-7. 10.3109/02770903.2010.485664
29 Heijkenskjöld-Rentzhog C, Kalm-Stephens P, Nordvall L, Malinovschi A, Alving K. New method for single-breath fraction of exhaled nitric oxide measurement with improved feasibility in preschool children with asthma. Pediatr Allergy Immunol. 2015 Nov;26(7):662-7. 10.1111/pai.12447
30 Jackson DJ, Virnig CM, Gangnon RE, Evans MD, Roberg KA, Anderson EL, et al. Fractional Exhaled Nitric Oxide (FeNO) Measurements are Most Closely Associated with Allergic Sensitization in School Aged Children. J Allergy Clin Immunol. 2009 Nov;124(5):949-53. 10.1016/j.jaci.2009.07.024
31 Vilmann L, Buchvald F, Green K, Nielsen KG. Fractional exhaled nitric oxide and multiple breath nitrogen washout in preschool healthy and asthmatic children. Respiratory Medicine. 2017 Dec 1;133:42-7. 10.1016/j.rmed.2017.10.027
32 Sayão LB, Britto MCA de, Burity E, Rattes C, Reinaux CMA, Fink J, et al. Exhaled nitric oxide as a diagnostic tool for wheezing in preschool children: A diagnostic accuracy study. Respiratory Medicine. 2016 Apr 1;113:15-21. 10.1016/j.rmed.2016.02.008
33 Blanco-Aparicio M, González-Barcala FJ, Padilla Galo A. [FeNO measurement devices]. Open Respir Arch. 2022;4(4):100207. 10.1016/j.opresp.2022.100207
34 Wyszyńska M, Nitsze-Wierzba M, Czelakowska A, Kasperski J, Żywiec J, Skucha-Nowak M. An Evidence-Based Review of Application Devices for Nitric Oxide Concentration Determination from Exhaled Air in the Diagnosis of Inflammation and Treatment Monitoring. Molecules. 2022 July 3;27(13):4279. 10.3390/molecules27134279
35 Darbà J, Ascanio M, Syk J, Alving K. Economic Evaluation of the Use of FeNO for the Diagnosis and Management of Asthma Patients in Primary Care in Sweden. Clinicoecon Outcomes Res. 2021 Apr 23;13:289-97. 10.2147/CEOR.S306389
36 Bonini M, Annibale R, Barbaglia S, Bo M, Capano F, Celeste M, et al. The role of Fraction Exhaled Nitric Oxide (FeNO) in asthma management: an Italian consensus statement on clinical and economic aspects. Multidiscip Respir Med. 2025 Apr 8;20(1):1006. 10.5826/mrm.2025.1006
37 Lewis G, Morton K, Santillo M, Yardley L, Wang K, Ainsworth B, et al. Qualitative insights into planning implementation of FeNO-guided asthma management in primary care. NPJ Prim Care Respir Med. 2025 Mar 20;35:16. 10.1038/s41533-025-00418-w
38 Buendía JA, Acuña-Cordero R, Rodriguez-Martinez CE. Cost utility of fractional exhaled nitric oxide monitoring for the management of children asthma. Cost Effectiveness and Resource Allocation. 2021 June 3;19(1):33. 10.1186/s12962-021-00287-3
39 Sabatelli L, Seppälä U, Sastre J, Crater G. Cost-effectiveness and Budget Impact of Routine Use of Fractional Exhaled Nitric Oxide Monitoring for the Management of Adult Asthma Patients in Spain. J Investig Allergol Clin Immunol. 2017;27(2):89-97. 10.18176/jiaci.0103
40 Fletcher MJ, Tsiligianni I, Kocks JWH, Cave A, Chunhua C, Sousa JC de, et al. Improving primary care management of asthma: do we know what really works? NPJ Prim Care Respir Med. 2020 June 17;30:29. 10.1038/s41533-020-0184-0
41 Harnan SE, Tappenden P, Essat M, Gomersall T, Minton J, Wong R, et al. The cost-effectiveness of FeNO testing for the diagnosis and management of asthma. In: Measurement of exhaled nitric oxide concentration in asthma: a systematic review and economic evaluation of NIOX MINO, NIOX VERO and NObreath [Internet]. NIHR Journals Library; 2015 [cited 2025 Aug 31]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK321828/
42 Rognoni C, Milano C, Heffler E, Bonini M, Brussino L, Carpagnano GE, et al. Economic impact of a more extensive use of FeNO testing on the Italian population with asthma. Respir Res. 2023;24:147. 10.1186/s12931-023-02437-y
43 Price D, Berg J, Lindgren P. An economic evaluation of NIOX MINO airway inflammation monitor in the United Kingdom. Allergy. 2009 Mar;64(3):431-8. 10.1111/j.1398-9995.2008.01855.x
44 El Abd A, Dasari H, Dodin P, Trottier H, Ducharme FM. The effects of vitamin D supplementation on inflammatory biomarkers in patients with asthma: a systematic review and meta-analysis of randomized controlled trials. Front Immunol. 2024 Mar 13;15:1335968. 10.3389/fimmu.2024.1335968
45 Lugogo N, Green CL, Agada N, Zhang S, Meghdadpour S, Zhou R, et al. Obesity’s effect on asthma extends to diagnostic criteria. J Allergy Clin Immunol. 2018 Mar;141(3):1096-104. 10.1016/j.jaci.2017.04.047
46 Anderson WJ, Short PM, Williamson PA, Lipworth BJ. Inhaled corticosteroid dose response using domiciliary exhaled nitric oxide in persistent asthma: the FENOtype trial. Chest. 2012 Dec;142(6):1553-61. 10.1378/chest.12-1310
47 Czubaj-Kowal M, Nowicki GJ, Kurzawa R, Polak M, Ślusarska B. Factors Influencing the Concentration of Exhaled Nitric Oxide (FeNO) in School Children Aged 8-9-Years-Old in Krakow, with High FeNO Values ≥ 20 ppb. Medicina (Kaunas). 2022 Jan 18;58(2):146. 10.3390/medicina58020146
48 Barański K, Kocot K, Melaniuk-Wolny E, Zajusz-Zubek E, Kowalska M. The Effect of Physical Activity on Spirometry and Fractional Exhaled Nitric Oxide in Adolescents-Longitudinal Study. Sustainability. 2021 Jan;13(11):5770. 10.3390/su13115770
49 Zhu Z, Xia S, Chen X, Guan WJ, Guo ZJ, Sun BQ. Factors associated with exhaled nitric oxide in children with asthma and allergic rhinitis. Clin Respir J. 2020 Jan;14(1):9-15. 10.1111/crj.13093
50 Jacinto T, Malinovschi A, Janson C, Fonseca J, Alving K. Evolution of exhaled nitric oxide levels throughout development and aging of healthy humans. J Breath Res. 2015 May 20;9(3):36005. 10.1088/1752-7155/9/3/036005
51 Wang D, Wang Y, Liang H, David JE, Bray CL. Race and ethnicity have significant influence on fractional exhaled nitric oxide. Ann Allergy Asthma Immunol. 2018 Mar;120(3):272-277.e1. 10.1016/j.anai.2017.11.021
52 Song WJ, Kim HJ, Shim JS, Won HK, Kang SY, Sohn KH, et al. Diagnostic accuracy of fractional exhaled nitric oxide measurement in predicting cough-variant asthma and eosinophilic bronchitis in adults with chronic cough: A systematic review and meta-analysis. J Allergy Clin Immunol. 2017 Sept;140(3):701-9. 10.1016/j.jaci.2016.11.037
53 Kunc P, Fabry J, Zatko T, Grendar M, Tatar M, Pecova R. Cough reflex sensitivity and fractional exhaled nitric oxide in children with asthma. Physiol Res. 2020 Dec 31;69(Suppl 3):S455-61. 10.33549/physiolres.934601
54 Maniscalco M, Ambrosino P, Poto R, Fuschillo S, Poto S, Matera MG, et al. Can FeNO be a biomarker in the post-COVID-19 patients monitoring? Respir Med. 2022 Mar;193:106745. 10.1016/j.rmed.2022.106745
55 Moeller A, Carlsen KH, Sly PD, Baraldi E, Piacentini G, Pavord I, et al. Monitoring asthma in childhood: lung function, bronchial responsiveness and inflammation. Eur Respir Rev. 2015 June;24(136):204-15. 10.1183/16000617.00003914
56 Oh MA, Shim JY, Jung YH, Seo JH, Young Kim H, Kwon JW, et al. Fraction of exhaled nitric oxide and wheezing phenotypes in preschool children. Pediatr Pulmonol. 2013 June;48(6):563-70. 10.1002/ppul.22705
57 Ferraro VA, Zanconato S, Baraldi E, Carraro S. Nitric Oxide and Biological Mediators in Pediatric Chronic Rhinosinusitis and Asthma. J Clin Med [Internet]. 2019 Oct 25 [cited 2020 Jan 6];8(11). Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6912805/
58 Caudri D, Wijga AH, Hoekstra MO, Kerkhof M, Koppelman GH, Brunekreef B, et al. Prediction of asthma in symptomatic preschool children using exhaled nitric oxide, Rint and specific IgE. Thorax. 2010 Sept;65(9):801-7. 10.1136/thx.2009.126912
59 Di Cara G, Marcucci F, Palomba A, Milioni M, Pecoraro L, Ciprandi G, et al. Exhaled nitric oxide in children with allergic rhinitis: a potential biomarker of asthma development. Pediatr Allergy Immunol. 2015 Feb;26(1):85-7. 10.1111/pai.12326
60 Xepapadaki P, Adachi Y, Pozo Beltrán CF, El-Sayed ZA, Gómez RM, Hossny E, et al. Utility of biomarkers in the diagnosis and monitoring of asthmatic children. World Allergy Organ J. 2022 Dec 15;16(1):100727. 10.1016/j.waojou.2022.100727
61 Wang X, Tan X, Li Q. Effectiveness of fractional exhaled nitric oxide for asthma management in children: A systematic review and meta-analysis. Pediatr Pulmonol. 2020 Aug; 55(8):1936-45. 10.1002/ppul.24898
62 Fraser A, Simpson R, Turner S. Use of exhaled nitric oxide in the diagnosis and monitoring of childhood asthma: myth or maxim? Breathe (Sheff). 2023 Dec;19(4):220236. 10.1183/20734735.0236-2022
63 Turner S, Cotton S, Wood J, Bell V, Raja EA, Scott NW, et al. Reducing asthma attacks in children using exhaled nitric oxide (RAACENO) as a biomarker to inform treatment strategy: a multicentre, parallel, randomised, controlled, phase 3 trial. The Lancet Respiratory Medicine. 2022 June 1;10(6):584-92. 10.1016/S2213-2600(21)00486-0
64 Hallas HW, Chawes BL, Rasmussen MA, Arianto L, Stokholm J, Bønnelykke K, et al. Airway obstruction and bronchial reactivity from age 1 month until 13 years in children with asthma: A prospective birth cohort study. PLoS Med. 2019 Jan;16(1):e1002722. 10.1371/journal.pmed.1002722
65 Dweik RA, Boggs PB, Erzurum SC, Irvin CG, Leigh MW, Lundberg JO, et al. An official ATS clinical practice guideline: interpretation of exhaled nitric oxide levels (FeNO) for clinical applications. Am J Respir Crit Care Med. 2011 Sept 1;184(5):602-15. 10.1164/rccm.9120-11ST
66 Horváth I, Barnes PJ, Loukides S, Sterk PJ, Högman M, Olin AC, et al. A European Respiratory Society technical standard: exhaled biomarkers in lung disease. Eur Respir J. 2017;49(4). 10.1183/13993003.00965-2016
67 Levy ML, Bacharier LB, Bateman E, Boulet LP, Brightling C, Buhl R, et al. Key recommendations for primary care from the 2022 Global Initiative for Asthma (GINA) update. NPJ Prim Care Respir Med. 2023 Feb 8;33(1):7. 10.1038/s41533-023-00330-1
68 Dinh-Thi-Dieu H, Vo-Thi-Kim A, Tran-Van H, Tang-Thi-Thao T, Duong-Quy S. Study of the beneficial role of exhaled nitric oxide in combination with GINA guidelines for titration of inhaled corticosteroids in children with asthma. J Breath Res. 2020 Mar 27;14(2):26014. 10.1088/1752-7163/ab6809
69 Karrasch S, Linde K, Rücker G, Sommer H, Karsch-Völk M, Kleijnen J, et al. Accuracy of FeNO for diagnosing asthma: a systematic review. Thorax. 2017 Feb;72(2):109-16. 10.1136/thoraxjnl-2016-208704
70 Pijnenburg MW. The Role of FeNO in Predicting Asthma. Front Pediatr. 2019;7:41. 10.3389/fped.2019.00041
71 Global Initiative for Asthma (GINA). Global Strategy for Asthma Management and Prevention 2024 [Internet]. 2024. Available from: https://ginasthma.org/wp-content/uploads/2025/05/GINA-2024-strategy-report_24_05_22-WMSA.pdf
72 Casale TB, Luskin AT, Busse W, Zeiger RS, Trzaskoma B, Yang M, et al. Omalizumab Effectiveness by Biomarker Status in Patients with Asthma: Evidence From PROSPERO, A Prospective Real-World Study. J Allergy Clin Immunol Pract. 2019 Jan;7(1):156-164.e1. 10.1016/j.jaip.2018.04.043
73 Jackson D, Shackshaft L, Green L, Roxas C, Fernandes M, Thompson L, et al. The relationship between fractional exhaled nitric oxide and asthma symptom scores in patients on mepolizumab. European Respiratory Journal [Internet]. 2019 Sept 28 [cited 2023 June 18];54(Suppl 63). Available from: https://erj.ersjournals.com/content/54/suppl_63/PA2623
74 Yancey SW, Keene ON, Albers FC, Ortega H, Bates S, Bleecker ER, et al. Biomarkers for severe eosinophilic asthma. J Allergy Clin Immunol. 2017 Dec;140(6):1509-18. 10.1016/j.jaci.2017.10.005
75 Shrimanker R, Keene O, Hynes G, Wenzel S, Yancey S, Pavord ID. Prognostic and Predictive Value of Blood Eosinophil Count, Fractional Exhaled Nitric Oxide, and Their Combination in Severe Asthma: A Post Hoc Analysis. Am J Respir Crit Care Med. 2019 Nov 15;200(10):1308-12. 10.1164/rccm.201903-0599LE
76 Murugesan N, Saxena D, Dileep A, Adrish M, Hanania NA. Update on the Role of FeNO in Asthma Management. Diagnostics. 2023 Jan;13(8):1428. 10.3390/diagnostics13081428
77 Busse WW, Wenzel SE, Casale TB, FitzGerald JM, Rice MS, Daizadeh N, et al. Baseline FeNO as a prognostic biomarker for subsequent severe asthma exacerbations in patients with uncontrolled, moderate-to-severe asthma receiving placebo in the LIBERTY ASTHMA QUEST study: a post-hoc analysis. Lancet Respir Med. 2021 Oct;9(10):1165-73. 10.1016/S2213-2600(21)00124-7
78 Castro M, Corren J, Pavord ID, Maspero J, Wenzel S, Rabe KF, et al. Dupilumab Efficacy and Safety in Moderate-to-Severe Uncontrolled Asthma. N Engl J Med. 2018 June 28;378(26):2486-96. 10.1056/NEJMoa1804092
79 Menzies-Gow A, Corren J, Bourdin A, Chupp G, Israel E, Wechsler ME, et al. Tezepelumab in Adults and Adolescents with Severe, Uncontrolled Asthma. New England Journal of Medicine. 2021 May 13;384(19):1800-9. 10.1056/NEJMoa2034975
80 Agache I, Beltran J, Akdis C, Akdis M, Canelo-Aybar C, Canonica GW, et al. Efficacy and safety of treatment with biologicals (benralizumab, dupilumab, mepolizumab, omalizumab and reslizumab) for severe eosinophilic asthma. A systematic review for the EAACI Guidelines-recommendations on the use of biologicals in severe asthma. Allergy. 2020 May;75(5):1023-42. 10.1111/all.14221