
Download

CASE REPORT
Delayed hypersensitivity reaction to cetirizine suggesting involvement of piperazine ring: a case report
Florence Libona*, Juliette Caronb, Anne Hermanc, A.F. Nikkelsa
aDepartment of Dermatology, CHU Liège, Sart Tilman, B-4000 Liège, Belgium
bDepartment of Allergology, Hôpital Saint Vincent de Paul, Lille, France
cDepartment of Dermatology, Cliniques Universitaires Saint-Luc, Université Catholique de Louvain (UC Louvain), and Department of Pneumology, Institute of Experimental and Clinical Research, LUNS Pole, Université Catholique de Louvain (UC Louvain), Brussels, Belgium
Abstract
Antihistamines (AHs) are widely prescribed for allergic conditions and are generally considered safe, with adverse reactions being rare. We report a case highlighting the possible involvement of piperazine ring in a delayed hypersensitivity reaction. A 25-year-old woman with a history of atopic dermatitis progressively developed a maculopapular drug eruption following intake of cetirizine. Patch testing was negative, but oral provocation with cetirizine reproduced the rash, confirming its causal role. Importantly, oral provocation with ciprofloxacin, which also contains a piperazine ring, elicited a similar reaction, supporting that this structural moiety itself was responsible for hypersensitivity. Alternatively, AHs lacking the piperazine ring, such as in bilastine and rupatadine, were well tolerated. This case provides the first direct evidence of delayed hypersensitivity manifesting as a maculopapular drug eruption, probably because of the piperazine ring, with cross-reactivity observed between structurally unrelated drugs. Clinicians should be aware of the potential for structural moiety-driven hypersensitivity to prevent recurrence across different drug classes.
Key words: antihistamines, cetirizine, delayed hypersensitivity, maculopapular rash, piperazine ring
*Corresponding author: Florence Libon, MD, PhD, Department of Dermatology, CHU Liège, Avenue de l’Hôpital 1, B-4000 Liège, Belgium. Email address: [email protected]
Received 31 August 2025; Accepted 5 November 2025; Available online 1 May 2026
Copyright: Libon F, et al.
This open access article is licensed under Creative Commons Attribution 4.0 International (CC BY 4.0). http://creativecommons.org/licenses/by/4.0/
Introduction
Antihistamines (AHs) are among the most commonly prescribed medications for allergic diseases. Their safety profile is generally excellent, with rare serious adverse reactions.1 Distinguishing drug-induced eruptions from flares of pre-existing dermatologic conditions, such as atopic dermatitis (AD), can be challenging, and standard diagnostic methods, including patch testing, often have limited sensitivity.2 Structural motifs, such as the piperazine ring present in cetirizine, may act as immunogenic trigger in delayed hypersensitivity reactions, yet their potential for cross-reactivity remains poorly characterized. In addition, excipients such as polyethylene glycol (PEG), frequently used in drug formulations, are implicated in hypersensitivity reactions and hence should be considered during the diagnostic work-up.3 Detailed case reports are therefore essential for advancing the understanding of clinical presentation, underlying mechanisms, and optimal diagnostic strategies. Importantly, identifying the causative molecular structure or excipient is crucial for patient care, as it guides the selection of alternative AHs and helps to prevent cross-reactions with medications from different drug classes.
Case report
A 25-year-old woman with a history of AD developed a generalized maculopapular rash (MPR) (Figure 1), without fever or systemic symptoms, gradually appearing 10 days after starting oral cetirizine (cetirizine® EG), 10 mg daily for allergic rhinitis. No other medications were taken. The eruption was clinically distinct from her usual AD flares. A skin biopsy revealed epidermal spongiosis with a superficial lymphomonocytic infiltrate while blood tests were normal. Cetirizine was discontinued, and oral methylprednisolone (32 mg/day with rapid tapering) was introduced, leading to complete remission within 1 week. The patient was closely monitored during the acute phase and for up to 10 days afterward to detect any delayed or systemic reactions. No such events occurred, and she subsequently tolerated her usual medications without incident. After 2 months, patch testing was performed using various AHs, each prepared in-house according to the recommended patch test guidelines2 (Table 1). The commercial form of each drug was diluted in petrolatum by following the European Society of Contact Dermatitis (ESCD) guidelines, which recommend using a 30% dilution for drug patch testing, except for desloratadine, which was tested at 1% according to the published recommendations of this specific drug.2 Ethylenediamine (ED) and PEG 400 (an excipient in Cetirizine® EG tablets), both obtained from chemotechnique (Vellinge, Sweden), were also tested, with PEG 400 prepared in a saline solution. All preparations were freshly prepared before application, which supports the reliability and stability of the reagents during testing. The haptens were applied on the back using Finn Chambers, and evaluations were performed at 48 and 72 h in accordance with the International Contact Dermatitis Research Group (ICDRG) criteria. No positive reactions were observed. An oral provocation test (OPT) with one-tenth of a cetirizine tablet induced a recurrence of the previous MPR after 7 days, incriminating cetirizine as a culprit of MPR. Additional provocation testing with PEG was not conducted, as the patient continued to take her usual PEG-containing medications after resolution of the rash, without recurrence of symptoms. Given the suspected involvement of the piperazine ring, a second OPT with ciprofloxacin (ciprofloxacin Sandoz®) was conducted, resulting in a comparable MPR, thereby supporting the causal role of this moiety. Alternative AHs, including bilastine and rupatadine, both devoid of piperazine ring structure, were well tolerated.
Table 1 Allergy workup performed in our patient.
| Test type | Substance | Result | Remarks |
|---|---|---|---|
| Patch test | Ethylenediamine (ED) 1% | − | |
| Polyethylene glycol (PEG) 400 | − | Present and tolerated in other patient’s medications | |
| Cetirizine 30% | − | ||
| Levocetirizine 30% | − | ||
| Desloratadine 1% | − | ||
| Rupatadine 30% | − | ||
| Ebastine 30% | − | ||
| Bilastine 30% | − | ||
| Intradermal tests | Not performed (absence of injectable cetirizinepreparations) | ||
| Oral provocation test | Cetirizine 10 mg (1/10 tablet) | + | Rash recurrence after 7 days |
| Bilastine 20 mg | − | ||
| Ebastine 10 mg | − | ||
| Ciprofloxacin 750 mg (1/10 tablet) | + | Rash recurrence after 7 days |
Figure 1 Maculopapular rashes (MPR) appearing 10 days after initiation of cetirizine treatment.
Discussion
Piperazine derivatives are the most frequent inducers of hypersensitivity among AHs, mainly affecting young to middle-aged females.1,4 Differentiating between AD flares and drug eruptions can be challenging as the cutaneous symptoms can mimic the underlying condition.4 The histopathological findings in our patient (mild spongiosis and superficial lymphocytic infiltrate) were consistent with those reported in maculopapular drug eruptions,5 and in the context of the recent introduction of cetirizine and the clinical presentation distinct from her usual AD flares, support the diagnosis of delayed drug hypersensitivity.
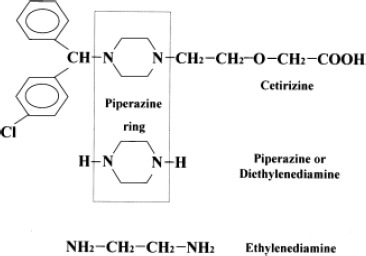
Cetirizine, similar to levocétirizine and hydroxyzine, contains a piperazine ring, structurally related to a cyclic dimer of ED, a stabilizer found in topical formulations (Figure 2).4,6,7 Despite being reported in previous case reports,8,9 piperazine patch testing could not be performed due to the absence of a validated and commercially available preparation. Although all patch tests in our patient were negative, a drug-related cause could not be excluded, given the limited positivity rate of patch testing for cutaneous adverse drug reactions, which range from 11% to 44%.2
Figure 2 Chemical structure of cetirizine, the piperazine ring, and ethylenediamine (ED).6
Antihistamines are poorly suited for native drug testing because of their hapten disposition and lack of standardized test reagents.4 Moreover, systemic AH therapy can activate the conformation of histamine receptors and cause adverse reactions that may not be detectable through skin testing.1 Intradermal tests were not performed: for cetirizine, no injectable formulation is currently available in Europe. Moreover, hydroxyzine, another AH containing a piperazine ring, is not widely available in injectable form, as availability varies across countries. Consequently, following the guidelines of the European Academy of Allergy and Clinical Immunology (EAACI),10 a drug provocation test with cetirizine was performed as the most reliable and feasible approach to establish a robust diagnosis, given a history suggestive of drug allergy, while other tests were inconclusive or unavailable.
For ciprofloxacin, skin tests with quinolones are controversial and results may be unreliable.11 In this context, a cautious oral provocation was performed, with close follow-up, using one-tenth of the usual cetirizine dose considering the severity of the initial eruption. The test reproduced the rash and confirmed the causal relationship. Subsequent reintroduction of ciprofloxacin elicited a similar reaction, demonstrating the role of the piperazine ring in the eruption, consistent with previously reported cross-reactivity in a bullous fixed drug eruption.12
Ciprofloxacin contains additional side chains beyond the piperazine ring that could potentially contribute to immunogenicity, and a similar consideration could apply to specific side chains of cetirizine. Nevertheless, the occurrence of hypersensitivity to both drugs in the same patient, which differ in overall structure but share a piperazine ring, supports the involvement of this common molecular feature. Given that the piperazine moiety is shared by numerous other drugs, including antipsychotics, antidepressants, antifungals, and certain cardiovascular medications,13 cross-reactivity related to this structural feature remains an important consideration to prevent future drug-induced reactions.
Conclusion
Cetirizine can rarely induce delayed hypersensitivity reactions, and diagnostic work-up should take into account both excipients (e.g., PEG-400) and the piperazine core. The observed cross-reactivity with ciprofloxacin provides support for the likely involvement of the piperazine ring, emphasizing the need for careful evaluation to prevent recurrence with structurally unrelated drug classes.
Mandatory Disclosure on Use of Artificial Intelligence
The authors declare that no AI-assisted tools were used in the preparation of this manuscript. All references have been manually verified for accuracy and relevance.
Author Contributions
All authors contributed equally to this article. All authors discussed the results and contributed to the final manuscript.
Conflict of Interest
The authors declared no potential conflict of interest with respect to research, authorship, and/or publication of this article. This article does not contain any individual person’s identifiable data; therefore, informed consent was not required.
Funding
None.
REFERENCES
1 Viñas M, Castillo MJ, Hernandez N, Ibero M. Cutaneous drug eruption induced by antihistamines. Clin Exp Dermatol. 2014;39:918–22. 10.1111/ced.12445
2 Barbaud A. Skin testing and patch testing in non-IgE-mediated drug allergy. Curr Allergy Asthma Rep. 2014;14:442. 10.1007/s11882-014-0442-8
3 Caballero ML, Quirce S. Delayed hypersensitivity reactions caused by drug excipients: A literature review. J Investig Allergol Clin Immunol. 2020;30(6):400–8. 10.18176/jiaci.0562
4 Shakouri AA, Bahna SL. Hypersensitivity to antihistamines. Allergy Asthma Proc. 2013;34:488–96. 10.2500/aap.2013.34.3699
5 Naim M, Weyers W, Metze D. Histopathologic features of exanthematous drug eruptions of the macular and papular type. Am J Dermatopathol. 2011;33:695–704. 10.1097/DAD.0b013e31820a285d
6 Cusano F. Clinicopathologic features of systemic contact dermatitis from ethylenediamine in cetirizine and levocetirizine. Dermatology. 2006;213:353–5. 10.1159/000096203
7 Piapan L, Belloni Fortina A, Giulioni E, Larese Filon F. Sensitization to ethylenediamine dihydrochloride in patients with contact dermatitis in northeastern Italy from 1996 to 2021. Contact Dermatitis. 2024;90:253–61. 10.1111/cod.14454
8 Lew BL, Haw CR, Lee MH. Cutaneous drug eruption from cetirizine and hydroxyzine. J Am Acad Dermatol. 2004;50: 953–6. 10.1016/j.jaad.2003.11.048
9 Stingeni L, Caraffini S, Agostinelli D, Ricci E, Lisi P. Maculopapular and urticarial eruption from cetirizine. Contact Dermatitis. 1997;37:249–50. 10.1111/j.1600-0536.1997.tb02456.x
10 Barbaud A, Garvey LH, Torres M, Laguna JJ, Arcolaci A, Bonadonna P, et al. EAACI/ENDA position paper on drug provocation testing. Allergy. 2024;79(3):565–79. 10.1111/all.15996
11 Zhu LJ, Liu AY, Wong PH, Arroyo AC. Road less traveled: Drug hypersensitivity to fluoroquinolones, vancomycin, tetracyclines, and macrolides. Clin Rev Allergy Immunol. 2022;62:505–18. 10.1007/s12016-021-08919-5
12 Alsubaiei F, Tétart F, Boulard C, Leblanc C, Joly P. Bullous fixed drug eruption to hydroxyzine and cross-reactivity with piperazine derivatives. Ann Dermatol Venereol. 2017;144:S139. 10.1016/j.annder.2017.09.187 (Article in French; English abstract available.)
13 Durand C, Szostak M. Recent advances in the synthesis of piperazines: Focus on C–H functionalization. Organics. 2021;2:337–47.1. 10.3390/org2040018