
Download
ORIGINAL ARTICLE
Alteration of triggers and symptoms by age group in childhood and adolescence anaphylaxis
Meltem Comerta*, Tugba Gulerb, Hasibe Artacc, Ilknur Kulhas Celikc
aKonya City Hospital, Department of Pediatrics, Division of Immunology and Allergy, Konya, Turkey
bErzurum City Hospital, Department of Pediatrics, Division of Immunology and Allergy, Erzurum, Turkey
cSelcuk University Medical Faculty, Department of Pediatrics, Division of Immunology and Allergy, Konya, Turkey
Abstract
Background: Anaphylaxis is a severe, potentially fatal, systemic hypersensitivity reaction induced by various triggers.
Objective: Only a few studies have examined the clinical manifestations of childhood anaphylaxis across different age groups. We aimed to evaluate, according to age group and trigger, the clinical features of anaphylaxis in pediatric patients.
Methods: We retrospectively evaluated 130 children diagnosed with anaphylaxis over 11 years.
Results: The median age of the patients was 10 years (min–max: 0.5–17.8), and 83 (63.8%) were male. Regarding age groups, 23 (17.7%) of the patients were infants, 26 (20%) were preschoolers, 31 (23.8%) were school-age children, and 50 (38.5%) were adolescents. Among the causes with known triggers, the most prevalent trigger was identified as food— affecting 44 (33.8%) cases—followed by drugs (34 cases, 26.2%) and venoms (18 cases, 13.8%). There was a statistically significant relationship between age groups and triggers (p < 0.001). The triggering role of drugs and venoms was found to be low in infants. Also, the infant group had significantly lower risks of venom-induced and drug-induced anaphylaxis compared to the adolescent group. The top three triggers identified in our patients were compared according to the system involved, and a statistically significant relationship was found between triggers and cardiovascular findings (p = 0.006).
Conclusion: The etiology of anaphylaxis may vary by age group. Depending on the trigger, it may also have different clinical manifestations.
Key words: allergens, anaphylaxis, children, etiology, diagnosis
*Corresponding author: Meltem Comert. Akabe Mah. Adana Çevre Yolu Cad. No. 135 42020 Karatay/KONYA. Email address: [email protected]
Received 19 May 2025; Accepted 30 August 2025; Available online 1 November 2025
Copyright: Comert M, et al.
This open access article is licensed under Creative Commons Attribution 4.0 International (CC BY 4.0). http://creativecommons.org/licenses/by/4.0/
Introduction
Anaphylaxis is a severe, potentially fatal, systemic hypersensitivity reaction that develops rapidly and is typically induced by various triggers, including food, drugs, and venoms.1 The epidemiological factors and triggers associated with anaphylaxis exhibit variation with age.1 Notably, drugs and venoms represent the most common causes of anaphylaxis in adults, whereas food allergy is the most common cause of anaphylaxis in children.1 The clinical manifestations of anaphylaxis are also dependent on triggers in children.2
Anaphylaxis is usually diagnosed if at least two organ systems are affected, with clinical manifestations including cutaneous, respiratory, cardiovascular, and gastrointestinal symptoms.3 In some cases, involvement of just one organ system (such as hypotension in the cardiovascular system) may be enough for diagnosis, and early adrenaline administration is fundamental for the management of anaphylaxis.3,4 There are currently no diagnostic criteria for anaphylaxis that are dependent on age.5 Diagnosing anaphylaxis in infants or toddlers can be challenging, as they may not be able to verbalize their symptoms, which may also be confused with normal infant conduct.5 Furthermore, adolescents differ from other age groups in their personal management of anaphylaxis because of the rapid and significant physical, emotional, and social changes that occur during this developmental period.6 A propensity for risk-taking, particularly among adolescents, has been identified as a contributing factor to the severity of reactions. This is predominantly associated with the underuse of adrenaline autoinjectors.7
There has been a notable increase in the incidence of anaphylaxis in children in recent years.1 However, only a few studies have examined the clinical manifestations of childhood anaphylaxis across different age groups. The objective of the present study is to evaluate, according to age group and trigger, the clinical features of anaphylaxis in pediatric patients diagnosed at our clinic.
Methods
Children diagnosed with anaphylaxis in the pediatric immunology and allergy unit of Selcuk University Faculty of Medicine Hospital between January 2012 and January 2023 were included in this study. Demographic features, detailed information on symptoms and signs, the triggering factor, the presence of an adrenaline autoinjector, the presence of concomitant allergic disease, the location of anaphylaxis occurrence, and the severity of anaphylaxis and treatments were recorded from patients’ files. Severity grading and diagnosis of anaphylaxis were based on criteria according to European Academy of Allergy and Clinical Immunology (EAACI) guidelines.3,8 The severity groups were categorized as follows: mild, moderate, and severe. In the absence of a proven causative agent, reactions were designated as idiopathic anaphylaxis. Patients aged between 0 and 18 years were included in the study and categorized into four groups based on their age at the time of diagnosis of anaphylaxis: over 12 (adolescents), 6–12 (school-age children), 3–5 (preschoolers), and 0–2 (infants) years. Ethical approval was acquired from the Institutional Ethical Review Board of Selçuk University (approval number: #2022/328).
Statistical methods
Statistical analyses were performed using IBM’s Statistical Package for the Social Sciences, version 23. The Shapiro–Wilk and Kolmogorov–Smirnov tests were used to verify the normality of variable distribution. The Mann–Whitney U test was used to compare nonnormally distributed data by groups of two or more. The Kruskal–Wallis H test was used to compare nonnormally distributed data by groups of three or more, and multiple comparisons were analyzed using the Dunn’s test. Fisher’s exact test, Yates’s correction, Pearson’s chi-squared test, and the Fisher–Freeman–Halton test were used to analyze the relationships between categorical data. The Bonferroni corrected Z-test was used for multiple comparisons of ratios. The impact of age groups on triggers and the duration of anaphylaxis were assessed using multinominal logistic regression analysis with odds ratio. Descriptors of quantitative data were presented as mean ± standard deviation and median (min–max) and categorical data as frequency (%). A p-value of <0.05 was considered statistically significant.
Results
One hundred and thirty children diagnosed with anaphylaxis were included in this study. The median age of the patients was 10 years (min–max: 0.5–17.8), and 83 (63.8%) were male. Regarding age groups, 23 (17.7%) of the patients were infants, 26 (20%) were preschoolers, 31 (23.8%) were school-age children, and 50 (38.5%) were adolescents. About 23.1% of patients were found to have idiopathic anaphylaxis. Fifty-nine (45.4%) patients developed anaphylaxis within the first 15 minutes, and 77 (59.2%) patients were administered adrenaline at the time of anaphylaxis. Furthermore, 30 (23.1%) patients had a previously prescribed adrenaline autoinjector before visiting our outpatient clinic. A total of 28 (21.5%) patients experienced anaphylaxis while at the hospital. Fifty-five (42.3%) patients had a concomitant allergic disease, of which the most common were allergic rhinitis (17.7%) and asthma (17.7%). The prevalence of mild anaphylaxis was 6.2%, moderate anaphylaxis was 64.6%, and severe anaphylaxis was 29.2%.
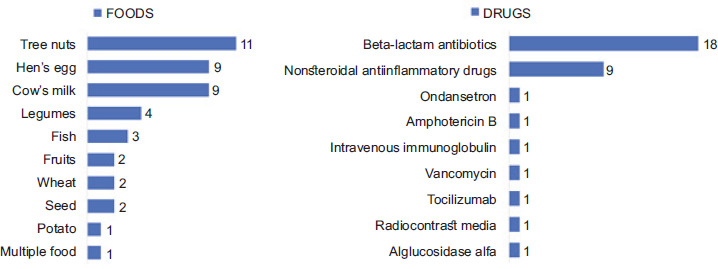
Among the causes with known triggers, the most prevalent trigger was identified as food—affecting 44 (33.8%) cases—followed by drugs (34 cases, 26.2%) and venoms (18 cases, 13.8%). Regarding the drug trigger, for 18 (52.9%) cases, it was beta-lactam antibiotics (BLAs), 9 (26.5%) cases with nonsteroidal anti-inflammatory drugs (NSAİDs), and 1 (2.9%) case each involving alglucosidase alfa, radiocontrast media, tocilizumab, vancomycin, intravenous immunoglobulin, amphotericin B, and ondansetron (Figure 1). The features of the patients are summarized in Table 1.
Table 1 Patient’s characteristics.
| Gender n, % | |
|---|---|
| Male | 83, 63.8% |
| Female | 47, 36.2% |
| Age at anaphlaxis (years) | 10 |
| Median (min-max) | (0.5-17.75) |
| Age groups n, % | |
| Infants | 23, 17.7% |
| Preschoolers | 26, 20% |
| School-age children | 31, 23.8% |
| Adolescents | 50, 38.5% |
| Triger n, % | |
| Food | 44, 33.8% |
| Drug | 34, 26.2% |
| Idiopathic | 30, 23.1% |
| Venom | 18, 13.8% |
| Other | 4, 3.1% |
| Duration of anaphylaxis development n, % | |
| 0-15 minutes | 59, 45.4% |
| 15-30 minutes | 15, 11.5% |
| 30-60 minutes | 19, 14.6% |
| >60 minutes | 7, 5.4% |
| Idiopathic | 30, 23.1% |
| Severity of anaphylaxis n, % | |
| Mild | 8, 6.2% |
| Moderate | 84, 64.6% |
| Severe | 38, 29.2% |
| The administration of adrenaline n, % | 77, 59.2% |
| Presence of adrenaline at outpatient | 30, 23.1% |
| visit n, % | |
| Area of anaphylaxis | |
| In hospital | 28, 21.5% |
| Out of hospital | 102, 78.5% |
| Concomitant allergic disease n, % | |
| Allergic rinitis | 23, 17.7% |
| Asthma | 23, 17.7% |
| Atopic dermatitis | 11, 8.5% |
| Allergic conjonktivitis | 5, 3.8% |
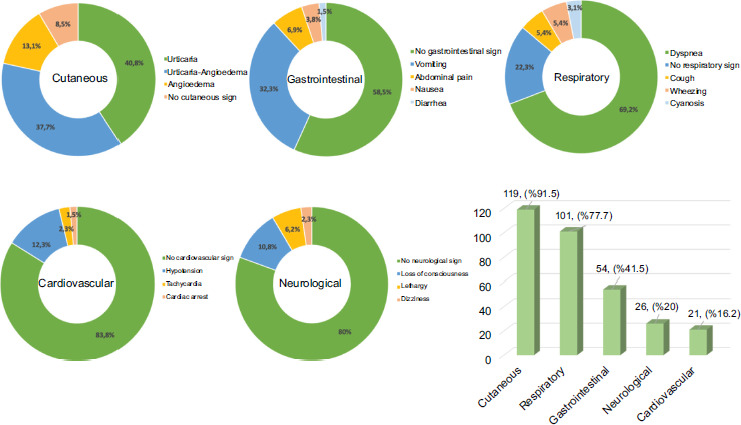
Regarding the food trigger, for 11 cases (25%), it was tree nuts; 9 (20.5%), hen eggs; 9 (20.5%), cow’s milk; 4 (9.1%), legumes; 3 (6.8%), fish; 2 (4.5%), fruits; 2 (4.5%), wheat; 2 (4.5%), seeds; 1 (2.3%), multiple foods; and 1 (2.3%), potatoes (Figure 1). The following clinical presentation was observed, listed in order of frequency: cutaneous (91.5%), respiratory (77.7%), gastrointestinal (41.5%), neurological (20%), and cardiovascular findings (16.2%). Figure 2 presents the detailed signs and symptoms during anaphylaxis.
Figure 1 Food and drug triggers of anaphylaxis.
Figure 2 Signs and symptoms during anaphylaxis.
There was a statistically significant relationship between age groups and triggers (p < 0.001) (Table 2). In the infant and preschool age groups, the most common trigger was identified as food (82.6% and 46.2%, respectively). In the adolescent age group, the idiopathic anaphylaxis was most prevalent, accounting for 38% of cases. The triggering role of drugs and venoms was found to be low in infants. A statistically significant relationship was observed between age groups and the duration of anaphylaxis (p = 0.023) (Table 2). The analysis revealed that most anaphylaxis cases occurred within the first 15 minutes in the infant, preschool, school, and adolescent age groups (60.9%, 46.2%, 51.6%, 34%, respectively). When we excluded cases of idiopathic anaphylaxis, the time interval between the onset of symptoms and anaphylaxis with a known allergen was 30 minutes in 74 cases (74%), and symptoms developed within the first 15 minutes in 59 patients (59%). Table 2 presents the characteristics of patients with anaphylaxis, categorized by age groups.
Table 2 Characteristics of patients with anaphylaxis categorized according to age groups.
| Age groups | Total | p | ||||
|---|---|---|---|---|---|---|
| Infants | Preschoolers | School-age children | Adolescents | |||
| Age median (min-max) | 1 (0.5-1.83)c | 3.58 (2.08-5.5)c | 10 (6-11.58)b | 15 (12-17.75)a | 10 (0.5-17.75) | <0.001*** |
| Gender n, (%) | ||||||
| Female | 6 (26.1) | 11 (42.3) | 9 (29) | 21 (42) | 47 (36.2) | 0.414* |
| Male | 17 (73.9) | 15 (57.7) | 22 (71) | 29 (58) | 83 (63.8) | |
| Trigger n, (%) | ||||||
| Food | 19 (82.6)a | 12 (46.2)b | 7 (22.6)b’c | 6 (12)c | 44 (33.8) | <0.001** |
| Drug | 1 (4.3)a | 10 (38.5)b | 8 (25.8)a’b | 15 (30)ab | 34 (26.2) | |
| Venom | 1 (4.3) | 1 (3.8) | 8 (25.8) | 8 (16) | 18 (13.8) | |
| Idiopathic | 0 (0)a | 3 (11.5)ab | 8 (25.8)b | 19 (38)b | 30 (23.1) | |
| Other | 2 (8.7) | 0 (0) | 0 (0) | 2 (4) | 4 (3.1) | |
| Severity of anaphylaxis n, (%) | ||||||
| Mild | 3 (13) | 1 (3.8) | 3 (9.7) | 1 (2) | 8 (6.2) | 0.268** |
| Moderate | 13 (56.5) | 19 (73.1) | 16 (51.6) | 36 (72) | 84 (64.6) | |
| Severe | 7 (30.4) | 6 (23.1) | 12 (38.7) | 13 (26) | 38 (29.2) | |
| Duration of anaphylaxis development n, (%) | ||||||
| 0-15 min | 14 (60.9) | 12 (46.2) | 16 (51.6) | 17 (34) | 59 (45.4) | 0.023** |
| 15-30 min | 4 (17.4) | 4 (15.4) | 1 (3.2) | 6 (12) | 15 (11.5) | |
| 30-60 min | 4 (17.4) | 6 (23.1) | 4 (12.9) | 5 (10) | 19 (14.6) | |
| >60 min | 1 (4.3) | 1 (3.8) | 2 (6.5) | 3 (6) | 7 (5.4) | |
| Idiopathic | 0 (0)a | 3 (11.5)ab | 8 (25.8)b | 19 (38)b | 30 (23.1) | |
| Cutaneous signs and | 19 (82.6) | 25 (96.2) | 28 (90.3) | 47 (94) | 119 (91.5) | 0.329** |
| symptoms n, (%) | ||||||
| Gastrointestinal signs and | 14 (60.9) | 13 (50) | 12 (38.7) | 15 (30) | 54 (41.5) | 0.067* |
| symptoms n, (%) | ||||||
| Respiratory signs and | 14 (60.9) | 20 (76.9) | 24 (77.4) | 43 (86) | 101 (77.7) | 0.124* |
| symptoms n, (%) | ||||||
| Cardiovascular signs and | 1 (4.3) | 2 (7.7) | 7 (22.6) | 11 (22) | 21 (16.2) | 0.113** |
| symptoms n, (%) | ||||||
| Neurological signs and | 7 (30.4) | 2 (7.7) | 8 (25.8) | 9 (18) | 26 (20) | 0.166** |
| symptoms n, (%) | ||||||
| The administration of | 15 (65.2) | 14 (53.8) | 16 (51.6) | 32 (64) | 77 (59.2) | 0.600* |
| adrenaline n, (%) | ||||||
Min-max: minimum-maximum; min: minute; *Pearson’s Chi-Square Test; **Fisher–Freeman–Halton Test; ***Kruskal–Wallis H Test, a–c. There is no difference between age groups with the same letter in each row.
The top three triggers identified in our patients were compared according to the system involved, and a statistically significant relationship was found between triggers and cardiovascular findings (p = 0.006). The prevalence rates of venom-induced anaphylaxis (VIA; 33.3%) and drug-induced anaphylaxis (DIA; 23.5%) were found to be higher than that of food-induced anaphylaxis (FIA; 4.5%) (Table 3). The features of patients with anaphylaxis categorized by trigger is illustrated in Table 3. The infant group had significantly lower risks of VIA and DIA compared to the adolescent group (OR: 0.039, 95% CI: 0.004–0.383; OR: 0.021, 95% CI: 0.002–0.194, respectively) (Table 4). The risk of developing VIA was also significantly lower in the preschool group compared to the adolescent group (OR: 0.063, 95% CI: 0.006–0.622) (Table 4). Table 4 presents the association of triggers with age groups.
Table 3 Characteristics of patients with anaphylaxis categorized according to trigger.
| Food | Drug | Venom | p | |
|---|---|---|---|---|
| Age median (min-max) | 2.17 (0.5-16)b | 11.25 (0.58-17.75)a | 11.54 (1.75-17)a | <0.001** |
| Gender n, (%) | ||||
| Female | 14 (31.8) | 16 (47.1) | 6 (33.3) | 0.356*** |
| Male | 30 (68.2) | 18 (52.9) | 12 (66.7) | |
| Duration of anaphylaxis development n, (%) | ||||
| 0-15 min | 22 (50) | 20 (58.8) | 14 (77.8) | 0.391* |
| 15-30 min | 6 (13.6) | 5 (14.7) | 3 (16.7) | |
| 30-60 min | 11 (25) | 7 (20.6) | 1 (5.6) | |
| >60 min | 5 (11.4) | 2 (5.9) | 0 (0) | |
| Idiopathic | 0 (0)a | 0 (0)a | 0 (0) | |
| Severity of anaphylaxis n, (%) | ||||
| Mild | 3 (6.8) | 3 (8.8) | 1 (5.6) | 0.124* |
| Moderate | 31 (70.5) | 18 (52.9) | 7 (38.9) | |
| Severe | 10 (22.7) | 13 (38.2) | 10 (55.6) | |
| Cutaneous signs and Symptoms n, (%) | 40 (90.9) | 32 (94.1) | 15 (83.3) | 0.422* |
| Gastrointestinal signs and Symptoms n, (%) | 19 (43.2) | 18 (52.9) | 7 (38.9) | 0.558*** |
| Respiratory signs and Symptoms n, (%) | 33 (75) | 26 (76.5) | 12 (66.7) | 0.750* |
| Cardiovascular signs and Symptoms n, (%) | 2 (4.5) | 8 (23.5) | 6 (33.3) | 0.006* |
| Neurological signs and Symptoms n, (%) | 7 (15.9) | 7 (20.6) | 8 (44.4) | 0.058* |
| The administration of Adrenaline n, (%) | 24 (54.5) | 22 (64.7) | 10 (55.6) | 0.642*** |
Min-max: minimum-maximum; min: minute; *Fisher–Freeman–Halton Test; ** Kruskal–Wallis H Test; *** Pearson’s Chi-Square Test, a–b. There is no difference between age groups with the same letter in each row.
Table 4 Association of triggers and duration of anaphylaxis development between age groups.
| Infants | Preschoolers | School-age children | |
|---|---|---|---|
| Trigger | OR (%95 CI) | OR (%95 CI) | OR (%95 CI) |
| Drug | 0.021 (0.002-0.194) | 0.333 (0.094-1.181) | 0.457 (0.114-1.831) |
| Venom | 0.039 (0.004-0.383) | 0.063 (0.006-0.622) | 0.857 (0.198-3.713) |
| Idiopathic | - | 0.079 (0.017-0.377) | 0.361 (0.092-1.417) |
| Other | 0.316 (0.036-2.75) | - | - |
| Duration of anaphylaxis development | OR (%95 CI) | OR (%95 CI) | OR (%95 CI) |
| 15-30 min | 0.81 (0.19-3.449) | 0.944 (0.218-4.088) | 0.177 (0.019-1.638) |
| 30-60 min | 0.971 (0.218-4.323) | 1.7 (0.42-6.881) | 0.85 (0.193-3.739) |
| >60 min | 0.405 (0.038-4.335) | 0.472 (0.044-5.106) | 0.708 (0.104-4.807) |
| Idiopathic | - | 0.224 (0.054-0.929) | 0.447 (0.153-1.306) |
OR: Odds ratio; CI: Confidence interval. The odds ratio was calculated for age groups, with the adolescent group as the reference. In terms of trigger types, the “food” trigger was taken as the reference, and in terms of the duration of anaphylaxis development, the “0–15 minutes” was taken as the reference.
Discussion
The present study constitutes an evaluation of pediatric anaphylaxis cases according to age and trigger over 11 years. As demonstrated in previous studies involving children,9,10 the present study found that more than half of the cases (83, 63.8%) were male. The role of gender in the pathogenesis of anaphylaxis remains to be elucidated.11 However, anaphylaxis manifests more frequently in boys until the age of 10–15 years; afterward, a higher incidence is observed in girls.10 The present study revealed a high male-to-female ratio in all groups, encompassing infants, preschool children, school-age children, and adolescents. The most prevalent findings were cutaneous symptoms (91.5%), followed by respiratory (77.7%), gastrointestinal (41.5%), neurological (20%), and cardiovascular (16.2%) findings. These findings are consistent with the literature.9,10
A multicenter study of Korean children revealed that food (74.7%) was the most frequent cause of anaphylaxis, followed by drugs and radiocontrast media (10.7%) and idiopathic factors (9.2%).12 A study conducted across Asia examined the etiology of anaphylaxis in 689 pediatric patients.13 The study revealed that food (62%) was the most prevalent trigger, followed by idiopathic factors (22%) and drugs (10%).13 Fifty-nine centers across Europe reported that in 889 children with anaphylaxis, food was responsible for 64.9% of cases, insect venom for 20.2%, and drugs for 4.8%.14 The findings of research conducted in two different Turkish cities indicated that the most prevalent causative agents, in order, were food, drugs, and venoms.9,15 We found that the most common trigger was food, followed by drugs, idiopathic factors, and venoms.
In the pediatric population, food is the most common cause of anaphylaxis.1 Furthermore triggers of anaphylaxis show geographical and age-related differences, underlining the significance of identifying causative factors based on regional data.16 A retrospective cross-sectional study conducted in Thailand over a 10-year period identified food as the most common trigger, with shrimp and fried insects being the predominant culprits.16 A study from Europe indicated that peanuts were the most prevalent food allergen, followed by wheat, hazelnut, hen’s egg and cow’s milk.14 In a 20-year retrospective study conducted in Italy, the most common foods associated with FIA were tree nuts (30%), milk (19%), eggs (15%), peanuts (12%), and fish and crustaceans (7%).10 In a study of 991 Korean pediatric patients with anaphylaxis, the top three food allergens were milk (28.4%), egg white (13.6%), and tree nuts (13.2%).12 In a study from Türkiye, the most commonly reported food allergens in pediatric patients with anaphylaxis were cow’s milk, tree nuts, and hen eggs (39.4%, 16% and 14.9%, respectively).9 The importance of tree nut allergy in general is that it is a lifelong condition, and it increases the risk of a severe reaction.17,18 In our study, among food allergies, the most trigger factor was tree nuts, followed by cow’s milk and hen eggs (25%, 20.5%, and 20.5%, respectively).
Another common cause of anaphylaxis is drugs. In the context of previous research on anaphylaxis in the pediatric population, DIA ranged widely from 5% to 33%.9 BLAs were the main causative agents in children with DIA in our study, a finding consistent with prior studies in children.9,12 Nonetheless, some studies revealed that NSAIDs were the most prevalent causative drugs.19,20 In the present study, in the category of drug allergies, the most prevalent trigger factor was identified as BLAs, followed by NSAİDs.
It is estimated that 1.5% to 34% of all cases of anaphylaxis are caused by venom.21 In our study, 13.8 % of anaphylaxis in pediatric patients are triggered by venom, which is slightly lower with the rates (15.9%–22.4%) reported in Türkiye.9,15 In the context of Türkiye and European populations, venoms have been identified as a significant contributing factor to anaphylaxis.9,14,15 Conversely, in Asia, VIA has been reported to be uncommon.13
There was a notable shift in triggers from food to venoms and drugs from infancy to early adolescence, after which the pattern of triggers was stable.22 Serbes et al.15 found that VIA and DIA are most common in children aged 7–11 years, while FIA is most common in infants under 1 year. Yagmur et al.9 showed that there was a decline in the prevalence of FIA from the infantile period to the adolescent period. Conversely, there was an increase in the prevalence of DIA, drugs being the most frequent trigger detected in the adolescent period.9 Another study from Türkiye corroborates the findings of other studies; as age increased, a decrease in the frequency of FİA was observed, while a concomitant increase in the rate of DİA was noted (p = 0.01 and p = 0.01, respectively).23 In our study, infants had significantly lower risks of DIA and VIA compared to the adolescent group. Tarczoñ et al. observed cardiovascular symptoms in all children with DIA studied and found that patients with VIA were significantly more likely to have cardiovascular symptoms than those with FIA.2 Serbes et al.15 also illustrated that DIA is associated with more cardiovascular involvement than FIA. We did not find any relationship between cardiovascular symptoms and age groups. In our study, DIA and VIA were very rare in infants, but cardiovascular symptoms were more frequently observed with these two forms of anaphylaxis.
The literature indicates that signs and symptoms of anaphylaxis generally appear within 30 minutes in the case of food allergies and even sooner in the case of parenteral drugs or insect stings.17 European data also reveal that 80.5% of reactions occur within 30 minutes after allergen exposure.14 In addition, they showed that the time interval between exposure and the onset of symptoms was found to be 55.1% within the first 10 minutes and 25.4% within 30 minutes after exposure.14 A comparison of groups of elicitors revealed that FIA appeared in a delayed pattern, with 13.9% of reactions occurring between 30 and 60 minutes, 7.9% until 2 hours after exposure to the allergen.14 A significant proportion of reactions that occurred at a late stage were reported in cases of anaphylaxis caused by drugs.14 Serbes et al. illustrated that the VIA was considerably quicker than drug and food triggers.15 In our study, the time interval between allergen exposure and the onset of symptoms was 15 minutes in 45.4% of all cases and 11.5% within 30 minutes. The present study has demonstrated that the duration of anaphylaxis in both DIA and FIA is found to be almost identical. Furthermore, it was demonstrated that VIA is marginally earlier than DIA and FIA. We found and a statistically significant relationship between age group and the duration of anaphylaxis development (p = 0.023) (Table 2).
Delayed use of adrenaline after anaphylaxis increases the risk of hospitalization and biphasic reactions, and most of those who die from anaphylaxis do not receive adrenaline in time.5 Prompt diagnosis and first-line treatment with adrenaline are crucial. Leung et al. reported that in 60% of anaphylaxis cases, adrenaline was administered.13 In Serbes et al.’s15 study, only 47.6% of children with anaphylaxis were given adrenaline. Our findings indicated that intramuscular adrenaline was administered at the time of anaphylaxis in 59.2% of cases, and only 23.1% of patients had prescribed adrenaline autoinjectors when they were referred to our outpatient clinic. We believe that increasing awareness of anaphylaxis among caregivers and healthcare professionals, as well as educating them on the prevention and management of anaphylaxis, will result in increased use of adrenaline autoinjectors.
The present study has several limitations. Firstly, it was retrospective, and secondly, the diagnosis of anaphylaxis was made on the basis of clinical findings. These limitations were mitigated by the following measures: the medical records of all patients were examined by the same allergy and immunology specialists in a standardized manner. There are only a limited number of studies in the literature reporting the alteration of triggers and symptoms by age group in childhood and adolescent anaphylaxis. We believe that our study makes a significant contribution to the literature.
In conclusion, the etiology of anaphylaxis may vary by age group. Depending on the trigger, it may also have different clinical manifestations. In the management and diagnosis of anaphylaxis, the usage of adrenaline and prescribed adrenaline autoinjectors in primary care should be increased through education of healthcare professionals.
Data Availability Statement
All data generated or analyzed during this study are included in this article and its supplementary material files. Further enquiries can be directed to the corresponding author.
Author Contributions
All authors contributed equally to this article.
Conflict of Interest
The authors declare no potential conflicts of interest with respect to research, authorship, and/or publication of this article.
Funding
None.
REFERENCES
1 Nagakura KI, Sato S, Asaumi T, Yanagida N, Ebisawa M. Novel insights regarding anaphylaxis in children—with a focus on prevalence, diagnosis, and treatment. Pediatr. Allergy Immunol. 2020;31(8):879–888. 10.1111/pai.13307
2 Tarczoń I, Jedynak-Wąsowicz U, Lis G, Tomasik T, Brzyski P, Cichocka-Jarosz E. Is the clinical manifestation of anaphylaxis in children influenced by the trigger of reaction? Postepy Dermatol. Alergol. 2021;38(5):788–797. 10.5114/ada.2020.95650
3 Muraro A, Worm M, Alviani C, Cardona V, DunnGalvin A, Garvey LH, et al. EAACI guidelines: anaphylaxis (2021 update). Allergy. 2022;77(2):357–377. 10.1111/all.15032
4 Navalpakam A, Thanaputkaiporn N, Poowuttikul P. Management of anaphylaxis. Immunol. Allergy Clin. North Am. 2022;42(1):65–76. 10.1016/j.iac.2021.09.005
5 Golden DBK, Wang J, Waserman S, Akin C, Campbell RL, Ellis AK, et al. Anaphylaxis: a 2023 practice parameter update. Ann. Allergy Asthma Immunol. 2024;132(2):124–176. 10.1016/j.anai.2023.09.015
6 Comberiati P, Spahn J, Peroni DG. Anaphylaxis in adolescents. Curr. Opin. Allergy Clin. Immunol. 2019;19(5):425–431. 10.1097/ACI.0000000000000572
7 Anagnostou K. Anaphylaxis in children: epidemiology, risk factors and management. Curr. Pediatr. Rev. 2018;14(3):180–186. 10.2174/1573396314666180507115115
8 Muraro A, Roberts G, Clark A, Eigenmann PA, Halken S, Lack G, et al. The management of anaphylaxis in childhood: position paper of the European Academy of Allergology and Clinical Immunology. Allergy. 2007;62(8):857–871. 10.1111/j.1398-9995.2007.01421.x
9 Turgay Yagmur I, Kulhas Celik I, Yilmaz Topal O, Civelek E, Toyran M, Karaatmaca B, et al. The etiology, clinical features, and severity of anaphylaxis in childhood by age groups. Int. Arch. Allergy Immunol. 2022;183(6):600–610. 10.1159/000521063
10 De Filippo M, Votto M, Albini M, Castagnoli R, De Amici M, Marseglia A, et al. Pediatric anaphylaxis: a 20-year retrospective analysis. J. Clin. Med. 2022;11(18):5285. 10.3390/jcm11185285
11 Salvati L, Vitiello G, Parronchi P. Gender differences in anaphylaxis. Curr. Opin. Allergy Clin. Immunol. 2019 Oct 19(5):417–424. 10.1097/ACI.0000000000000568
12 Lee SY, Ahn K, Kim J, Jang GC, Min TK, Yang HJ, et al. A multicenter retrospective case study of anaphylaxis triggers by age in Korean children. Allergy Asthma Immunol. Res. 2016;8(6):535–540. 10.4168/aair.2016.8.6.535
13 Leung ASY, Tham EH, Pacharn P, Xing Y, Trinh HKT, Lee S, et al. Disparities in pediatric anaphylaxis triggers and management across Asia. Allergy. 2024;79(5):1317–1328. 10.1111/all.16098
14 Worm M, Moneret-Vautrin A, Scherer K, Lang R, Fernandez-Rivas M, Cardona V, et al. First European data from the network of severe allergic reactions (NORA). Allergy. 2014;69(10):1397–1404. 10.1111/all.12475
15 Serbes M, Sasihuseyinoglu AS, Ozcan D, Ufuk Altıntas D. Clinical features of anaphylaxis in children. Allergy Asthma Proc. 2022;43(1):50–56. 10.2500/aap.2022.43.210089
16 Uthaisangsook S, Hirunwattana N, Kajornrojanaruk C, Padsee N. Characteristics of anaphylaxis from a tertiary-care hospital in lower northern Thailand: a ten-year retrospective cross-sectional study. Asian Pac. J. Allergy Immunol. 2024. doi:10.12932/AP-010424-1831
17 Muraro A, Roberts G, Worm M, Bilò MB, Brockow K, Fernández Rivas M, et al. Anaphylaxis: guidelines from the European Academy of Allergy and Clinical Immunology. Allergy. 2014;69(8):1026–1045. 10.1111/all.12437
18 Cetinkaya PG, Buyuktiryaki B, Soyer O, Sahiner UM, Sekerel BE. Factors predicting anaphylaxis in children with tree nut allergies. Allergy Asthma Proc. 2019;40(3):180–186. 10.2500/aap.2019.40.4211
19 Nunes FA, Zanini F, Braga CS, da Silva AL, Fernandes FR, Solé D, et al. Incidence, triggering factors, symptoms, and treatment of anaphylaxis in a pediatric hospital. World Allergy Organ. J. 2022;15(9):100689. 10.1016/j.waojou.2022.100689
20 Sole D, Ivancevich JC, Borges MS, Coelho MA, Rosario NA, Ardusso L, et al. Anaphylaxis in Latin American children and adolescents: the online Latin American survey on anaphylaxis (OLASA). Allergol. Immunopathol. 2012; 40(6): 331–5. 10.1016/j.aller.2011.09.008
21 Yu JE, Lin RY. The epidemiology of anaphylaxis. Clin. Rev. Allergy Immunol. 2018; 54(3):366–74. 10.1007/s12016-015-8503-x
22 Grabenhenrich LB, Dölle S, Moneret-Vautrin A, Köhli A, Lange L, Spindler T, et al. Anaphylaxis in children and adolescents: the European Anaphylaxis Registry. J. Allergy Clin. Immunol. 2016 Apr 137(4):1128-1137.e1. 10.1016/j.jaci.2015.11.015
23 Celiksoy MH, Ulas S, Turan I, Yıldırım I, Ucar OT, Al S. Characteristics of childhood anaphylaxis in different age groups. Allergol Immunopathol. 2024; 52(5): 1–5. 10.15586/aei.v52i5.1131