
Download
ORIGINAL ARTICLE
Prevalence and triggers of allergic diseases across different age groups: A comparative analysis of patients aged under 50, 50–64, and 65 and older
Alper Ekinci, Seda Altiner*
Department of Immunology and Allergy, Ankara University Faculty of Medicine, Ankara, Türkiye
Abstract
Allergic diseases are prevalent immune disorders that have a considerable impact on public health. Although these cases are traditionally linked with younger individuals, older populations are increasingly affected due to immunological changes and a greater prevalence of comorbidities. The aim of this study was to evaluate the prevalence and triggers of allergic diseases across three age groups—under 50, 50–64, and 65 and older—to inform age-specific prevention and treatment strategies. In this retrospective study, data from 352 patients (270 females and 82 males) who presented to our allergy clinic between December 2022 and December 2023 were analyzed. Patients were grouped by age and data on allergic diseases, triggers, comorbidities, and skin prick test results were evaluated. Appropriate statistical analyses were performed, with statistical significance defined as p < 0.05. Allergic rhinitis (39.8%) was the most prevalent allergic disease, followed by chronic spontaneous urticaria (28.1%), and acute urticaria-angioedema (27.8%). Drug allergies were significantly more frequent in older adults (p = 0.016), with nonsteroidal anti-inflammatory drugs and beta-lactam antibiotics being common triggers. Allergic rhinitis was more prevalent in the < 50 age group (p = 0.013). Skin prick tests revealed sensitivities to pollen (9.4%), house dust mites (8.8%), and cat allergens (2.8%). Allergic diseases vary in frequency across age groups. Allergic rhinitis is more common in younger patients, while drug allergies are dominant in the elderly, likely due to polypharmacy. Raising awareness and tailoring diagnostic approaches for allergic diseases in older adults is essential. Further multicenter studies are needed to confirm these findings.
Key words: allergy, age, elder, prevalence, trigger
*Corresponding author: Seda Altiner, Department of Immunology and Allergy, Ankara University Faculty of Medicine, Ankara, Türkiye. Email address: [email protected]
Received 24 April 2025; Accepted 12 August 2025; Available online 1 November 2025
Copyright: Ekinci A. and Altiner S.
This open access article is licensed under Creative Commons Attribution 4.0 International (CC BY 4.0). http://creativecommons.org/licenses/by/4.0/
Introduction
Allergic diseases are among the most common immune system disorders in society and constitute a significant health problem in developed countries.1 While allergic diseases are primarily considered a health concern for the younger age group, as the population ages and life expectancy increases among older individuals, it is expected that allergic diseases will be observed at increasing rates in the elderly population as well.1 Additionally, in developed societies, the incidence of allergic diseases is on the rise due to various factors, including climate change, air pollution, and changes in dietary habits.1 During the aging process, significant changes occur in the functioning of the immune system, including alterations in the proportions of lymphocyte subsets, defects in apoptosis processes, mitochondrial functions, and stress responses.1 In line with this, in elderly individuals, the shift of the immune response toward the T helper 2 direction may lead to increased susceptibility to infections, along with the easier occurrence of neoplastic diseases, metabolic disorders, and allergic diseases.1 Furthermore, it was reported that due to modifications in the interactions between different components of the immune system such as cellular and humoral immunity or natural and acquired immunity, chronic inflammation and the development of allergies may occur more easily in elderly individuals1; however, different studies also emphasized that allergic diseases may decrease in incidence as a result of immunosenescence.2
In the literature, the middle-aged group is defined as 50–64 years old, while the elderly group is defined as 65 years and older.3 There are studies in the literature suggesting that the frequencies of various allergic diseases may vary across different age groups.4 Changes observed in the immune system as age advances, coupled with the presence of various comorbidities in older age leading to the use of multiple medications, result in considerable differences in the diagnosis and treatment of allergic diseases in the elderly compared to younger age groups.4 The diagnosis of various allergic diseases in elderly individuals can be easily overlooked due to differences in clinical manifestations compared to the younger age group as well as the bias that allergic diseases are primarily a concern for the younger population. Therefore, it was highlighted that specialized approaches are needed for the diagnosis of allergic diseases in elderly individuals.4,5
We aimed to examine the distribution of types of allergic diseases and the distribution of factors to which patients are sensitive according to age groups of patients aged 65 and over, 50– 64 years, and under 50 years who presented to our outpatient clinic. Our aim was to contribute to the literature by comparing these results to the results of other studies and developing different preventive and therapeutic strategies tailored to different age groups. Such investigations can provide valuable insights into developing age-specific preventive and therapeutic strategies, guiding clinical practice, and enhancing the understanding of immunological changes during the aging process.
Materials and Method
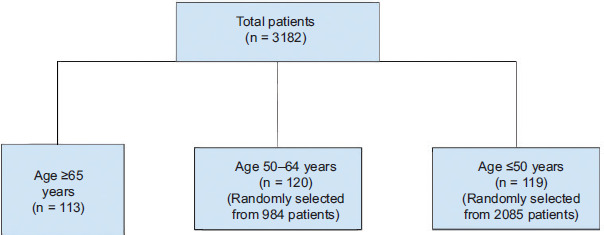
In this retrospective study, we reviewed the records of a total of 3182 patients who visited our clinic between December 1, 2022, and December 1, 2023. During this period, there were 113 elderly patients and whose information regarding patient records could be fully accessed. All individuals aged over 65 years who visited the outpatient clinic within a 1-year period were included using a total population sampling approach, as the group size was relatively limited. Additionally, through randomization, 119 patients under the age of 50 and 120 middle-aged patients were selected from among the 2085 patients under 50 and 984 middle-aged patients who visited our clinic during the same period. For the age groups between 50 and 65 years and under 50 years, the simple random sampling method was employed to ensure comparability across age categories. Specifically, from each of these two larger age groups, participants were randomly selected to match the sample size of the ≥ 65 age group. Randomization was performed using computer-generated random numbers in Microsoft Excel where each eligible patient was assigned a random number and the dataset was sorted accordingly. The first 119 patients under the age of 50 and 120 middle-aged patients were then selected. This approach ensured that selection bias was minimized and where each individual within the age groups had an equal probability of being included in the study. The flowchart of the patient selection process employed in the study is presented in Figure 1. Data regarding the patients, including age, sex, type of allergic disease, triggering factors of the disease, additional systemic diseases, and results of skin prick tests, were obtained.
Figure 1 Flowchart for patient selection.
Before starting the study, we obtained the necessary approval from the ethics committee of our institution.
Statistical analyses were conducted using the IBM® SPSS (Statistical Package for the Social Sciences) version 27 software. Descriptive statistics are presented as frequency and percentage values for the categorical variables and median (minimum-maximum) or mean ± standard deviation (SD) values for the continuous variables. Independent group comparisons for the categorical variables were performed using chi-squared or Fisher’s exact tests, where applicable. The normality of the distribution of continuous variables was assessed visually (histograms and probability plots) and analytically (Kolmogorov-Smirnov/Shapiro-Wilk tests). The continuous variables were analyzed using Student’s t-test or Mann-Whitney U test, depending on the distribution for comparisons between two independent groups. For comparisons involving more than two independent groups, one-way analysis of variance (ANOVA) or the Kruskal-Wallis test was used. A significance level of 0.05 (5%) was chosen for statistical significance (Type I error rate).
Results
The sample for this study included 352 patients, of whom 270 (76.7%) were females and 82 (23.3%) males. The most commonly diagnosed allergic condition was allergic rhinitis, affecting 39.8% (n = 140) of the patients, followed by chronic spontaneous urticaria (28.1%, n = 99) and acute urticaria-angioedema (27.8%, n = 98). Among the acute urticaria-angioedema cases, drugs were the most frequently identified triggers (16.5%, n = 58), while food-related triggers and unidentified causes accounted for 5.7% (n = 20) each. Drug hypersensitivity reactions were reported in 22.2% (n = 78) of the sample and were predominantly manifested as urticaria-angioedema (16.5%, n = 58), with smaller proportions presenting as anaphylaxis (4.3%, n = 15) and maculopapular drug eruptions (1.4%, n = 5). The most frequently implicated agents included nonsteroidal anti-inflammatory drugs (NSAIDs) and beta-lactam antibiotics (each 8.2%, n = 29), in addition to non-beta-lactam antibiotics (5.4%, n = 19) and radiographic contrast media (2.3%, n = 8). Less commonly, other drugs accounted for an additional 4% (n = 14) of the reported reactions. The prevalence of asthma was determined to be 9.1% (n = 32). Anaphylaxis was observed in 5.7% (n = 20) of the patients, mainly attributed to drugs (4.3%, n = 15) and Hymenoptera venom (1.1%, n = 4), with one idiopathic case (0.28%, n = 1). Comorbid conditions were documented in 46.7% (n = 164) of the patients, with the most common comorbid conditions being hypertension (28.5%, n = 100), diabetes mellitus (17.4%, n = 61), hypothyroidism (11.7%, n = 41), and hyperlipidemia (8%, n = 28). The main data regarding demographic and clinical characteristics are presented in Table 1.
Table 1 Demographic and clinical characteristics of the patients.
| Variable | n (%) |
|---|---|
| Total Number of Patients (n) | 352 |
| Male | 82 (23.3%) |
| Female | 270 (76.7%) |
| Patients with Allergic Rhinitis | 140 (39.8%) |
| Patients with Chronic Spontaneous Urticaria | 99 (28.1%) |
| Patients with Acute Urticaria-Angioedema (any cause) | 98 (27.8%) |
| Patients with Drug Allergy | 78 (22.2%) |
| Urticaria-Angioedema | 58 (16.5%) |
| Anaphylaxis | 15 (4.3%) |
| Maculopapular Drug Eruption | 5 (1.4%) |
| Patients with Asthma | 32 (9.1%) |
| Patients with Anaphylaxis (any cause) | 20 (5.7%) |
| Patients with Comorbidities | 164 (46.7%) |
| Hypertension | 100 (28.5%) |
| Diabetes Mellitus | 61 (17.4%) |
| Hypothyroidism | 41 (11.7%) |
| Hyperlipidemia | 28 (8%) |
Skin prick testing was performed in 43.5% of the patients (n = 153). Sensitization was most frequently observed to pollen (9.4%, n = 33) and house dust mites (8.8%, n = 31), with lower rates for cat (2.8%, n = 10) and mold allergens (1.1%, n = 4). The mean wheal diameter induced by components on the skin prick test was 7.02 ± 1.33 mm for histamine, 7.58 ± 2.56 mm for pollen, 4.13 ± 1.73 mm for house dust mites, 4.30 ± 1.77 mm for cat allergens, and 3 ± 0 mm for mold allergens.
While sex distribution remained similar across age groups (p = 0.875), the prevalence of allergic rhinitis decreased significantly with age—50.4% (n = 60) in those under 50 years, 35.8% (n = 43) in those 50– 65 years, and 32.7% (n = 37) in those aged 65 and older (p = 0.013). In contrast, drug allergies showed an age-related increase, rising from 13.4% (n = 16) in the youngest group, 25% (n = 30) in the middle-aged group, to 28.3% (n = 32) in the oldest group (p = 0.016). Urticaria-angioedema remained the predominant drug allergy phenotype across all age categories, with no significant age-related variation in the distribution of clinical manifestations (p > 0.05). No significant differences were observed among age groups in terms of the prevalence of chronic spontaneous urticaria (p = 0.180), acute urticaria-angioedema (p = 0.857), asthma (p = 0.479), or anaphylaxis (p = 0.684).
The presence of comorbidities was observed in 15.1% (n = 18) of the group under 50 years old, 52.5% (n = 63) in the middle-aged group, and 74.1% (n = 83) in the elderly group. A statistically significant difference was found in the frequency of comorbidities among the included age groups (p < 0.001).
The data regarding the comparison of patients according to age groups are presented in Table 2.
Table 2 Comparisons of the patients according to age groups.
| Variable | < 50 Years (n = 119) | 50-64 Years (n = 120) | > 65 Years (n = 113) | P0 | P1 | P2 | P3 |
|---|---|---|---|---|---|---|---|
| Sex (Male), n (%) | 28 (23.5%) | 26 (21.7%) | 28 (24.8%) | 0.875 | 0.730 | 0.824 | 0.573 |
| Sex (Female), n (%) | 91 (76.5%) | 94 (78.3%) | 85 (75.2%) | ||||
| Allergic Rhinitis, n (%) | 60 (50.4%) | 43 (35.8%) | 37 (32.7%) | 0.013 | 0.022 | 0.006 | 0.620 |
| Chronic Spontaneous Urticaria, n (%) | 27 (22.7%) | 33 (28.3%) | 38 (33.6%) | 0.180 | 0.391 | 0.060 | 0.310 |
| Drug Allergy, n (%) | 16 (13.4%) | 30 (25.0%) | 32 (28.3%) | 0.016 | 0.023 | 0.005 | 0.567 |
| Urticaria-Angioedema | 13 (10.9%) | 24 (20.0%) | 21 (18.6%) | 0.128 | 0.052 | 0.099 | 0.784 |
| Anaphylaxis | 3 (2.5%) | 5 (4.2%) | 7 (6.2%) | 0.562 | 0.722 | 0.206 | 0.484 |
| Maculopapular Eruption | 0 (0.0%) | 1 (0.8%) | 4 (3.5%) | 0.207 | 1.000 | 0.055 | 0.201 |
| Acute Urticaria-Angioedema | 31 (26.1%) | 34 (28.3%) | 33 (29.2%) | 0.857 | 0.692 | 0.592 | 0.882 |
| (any cause), n (%) | |||||||
| Asthma, n (%) | 9 (7.6%) | 14 (11.7%) | 9 (8.0%) | 0.479 | 0.282 | 0.909 | 0.344 |
| Anaphylaxis (any cause), n (%) | 5 (4.2%) | 8 (6.7%) | 7 (6.2%) | 0.684 | 0.401 | 0.493 | 0.882 |
| Comorbidities, n (%) | 18 (15.1%) | 63 (52.5%) | 83 (74.1%) | <0.001 | <0.001 | <0.001 | <0.001 |
p0 : Statistical comparison of all three groups.
p1 : Statistical comparison of the <50 years and 50–64 years groups.
p2 : Statistical comparison of the <50 years and ≥65 years groups.
p3 : Statistical comparison of the 50–64 years and ≥65 years groups.
Discussion
In our study, we examined the distribution of different types of allergic diseases among age groups in allergy patients who visited our clinic within one year. To the best of our knowledge, our study is the first to compare the frequency of allergic diseases in the elderly patient group to those in the middle-aged and under-50 groups.
In our study, the most frequently observed diseases among the patients were allergic rhinitis, chronic spontaneous urticaria, acute urticaria-angioedema, and drug allergy, respectively. The prevalence of allergic rhinitis in adults is typically between 10% and 30%.6 It was reported that chronic urticaria affected approximately 1– 2% of the general population,7 and that approximately 20% of the general population experienced at least one episode of acute urticaria throughout their lifetime.8 The frequency of adverse drug reactions in hospitalized cases is 15%.9 Penicillin derivative antibiotics are among the most common drug groups causing allergies in the population, with approximately 10% of patients describing penicillin allergy. However, it was found that 90% of these cases are not truly allergic.10 In this context, it can be considered difficult to determine the true prevalence of drug allergies in a population.
Urticaria is generally associated with mast cells located superficially and deep in the dermis, and various mediators, including histamine primarily found in mast cell granules, play a role in the development of the condition.11 Its main clinical manifestation is raised, itchy, and erythematous lesions on the skin that regress within 24 hours without leaving a trace.11 In some cases, angioedema, characterized by swelling on mucosal surfaces, especially on the lips and eyelids, accompanies the condition.11 Acute urticaria lasts for less than 6 weeks, while chronic urticaria lasts for more than 6 weeks.11 The development of chronic urticaria from acute urticaria is rare; therefore, acute urticaria and chronic urticaria are considered distinct disease entities.11 Acute urticaria can generally be triggered by viral infections, foods, and medications, although the triggering factor cannot be identified in many cases.11 Chronic urticaria develops not due to an external allergen, but rather as a result of intrinsic immune mechanisms leading to mast cell degranulation.11 The most common triggers of acute urticaria-angioedema cases evaluated in our clinic were found to be medications, followed by foods. In this context, the findings of our study were consistent with the literature.
Drug reactions are classified in the literature as immediate-type and delayed-type reactions. Immediate-type reactions such as urticaria, angioedema, and anaphylaxis typically develop within 1–6 hours after drug intake,9 and delayed-type reactions can however develop days after exposure to the drug.9 In general, the pathogenesis of immediate-type reactions involves immunoglobulin E (IgE) and mast cells, while the pathogenesis of delayed-type reactions involves IgG and T lymphocytes, depending on the type of reaction.9 In the literature, the most common types of cutaneous drug reactions were reported as maculopapular drug eruption and urticaria, respectively.12 Severe reactions, including drug-related eosinophilia with systemic symptoms syndrome (DRESS), acute generalized exanthematous pustulosis (AGEP), Stevens-Johnson syndrome (SJS), and toxic epidermal necrolysis (TEN), can also occur, albeit less frequently.9
In the literature, allergic reactions have been observed with a wide variety of drugs, including penicillin derivative antibiotics, other antibiotics, NSAIDs , antiepileptic drugs, and many others.13
Our results showed that the most commonly observed clinical presentations in the patients were urticaria-angioedema, anaphylaxis, and maculopapular drug eruption, respectively. Although previous studies have reported a higher incidence of maculopapular drug eruptions, one reason for the more frequent observation of clinical presentations associated with immediate-type hypersensitivity in our study might be that these patients tend to present more prominently to dermatology clinics for differentiation from other dermatological diseases, including viral exanthems, which can mimic maculopapular drug eruptions, leading to fewer referrals to our clinic. Additionally, in our study, the most common triggers of drug allergies were found to be NSAIDs and beta-lactam antibiotics, which was consistent with literature data.
Allergic rhinitis is a condition characterized by the development of symptoms such as sneezing, nasal discharge, nasal congestion, and itching due to a type 1 hypersensitivity response observed in the nasal mucosa following exposure to various respiratory allergens.14 The symptoms and signs of the disease occur as a result of mast cell degranulation triggered by the binding of allergen-specific IgE present on the nasal mucosa to the responsible allergen.14 In the literature, the most commonly implicated aeroallergens in the development of allergic rhinitis are dust mites, various pollens, animal dander, and molds.15 In a recent study, the most common aeroallergens were found to be dust mites, pollens, storage mites, cockroaches, molds, and cat and dog epithelium residues, respectively. The results of the same study suggested that the frequency and distribution of aeroallergens may vary regionally.15 In our study, the most common sensitivities detected in patients undergoing skin prick tests were pollen, dust mites, cat dander, and mold allergens, respectively.
The most commonly affected age group for allergic rhinitis was reported to be between the second and fourth decades of life, with symptoms typically starting before the age of 20 in most cases.14 The age range in which acute urticaria can occur is typically 3 months to 88 years old, and most cases are observed in their 20s.16 Chronic urticaria is most commonly reported to occur between the ages of 25 and 55.17 In a recent study, the age group with the highest incidence of drug allergy was found to be 50– 59-year olds; however, it had also shown that the cumulative incidence of drug allergy increases with age.18
In our study, allergic rhinitis, acute urticaria-angioedema, chronic spontaneous urticaria, and drug allergy were the most commonly observed allergic diseases for those under 50 and the middle-aged group, respectively. In the elderly group, the most commonly observed allergic diseases were chronic spontaneous urticaria, allergic rhinitis, acute urticaria-angioedema, and drug allergies, respectively. Therefore, it can be considered that allergic diseases commonly observed in individuals under 50 and in the middle-aged group may also be present in elderly individuals; hence, raising awareness for the diagnosis of allergic diseases in the elderly population may be necessary. The ranking of various allergic diseases in our study differed from those in other studies in the relevant literature, which could be attributed to different studies reporting varying frequencies of different diseases and the possibility of our cases showing different distributions compared to the general population, as they were referred to our clinic instead of being representative of the general population. Additionally, some cases may have been evaluated in different specialty clinics instead of presenting to our clinic, which could have contributed to the different distribution of cases in our study.
On the one hand, in the comparisons of the frequencies of allergic diseases among age groups, allergic rhinitis was significantly more common in the under 50 and middle-aged groups compared to the elderly group. On the other hand, drug allergies were significantly more common in the elderly group compared to the under 50 and middle-aged groups. Various studies have emphasized that the prevalence of allergic rhinitis is lower in elderly individuals compared to younger individuals.2 It was noted that the higher frequency of medication use and polypharmacy in elderly individuals may contribute to a higher incidence of drug allergy in this age group.5 In our study, the frequency of comorbidities in the elderly group was significantly higher compared to the middle-aged and the under 50 groups. In line with this, the higher incidence of drug allergies in the elderly group in our study was consistent with the information in the literature.
The main limitations of our study include being a single-center and retrospective study as well as the involvement of a relatively small number of patients presenting to our clinic within a limited time frame. These limitations may reduce the generalizability of the results of our study. More enlightening results regarding the frequency and distribution of allergic diseases in the elderly population compared to younger and middle-aged population could be obtained through larger scale, multicenter, and prospective studies involving greater numbers of participants.
Conclusion
Our results indicate that various allergic diseases observed in individuals under 65 years of age can also be observed in elderly individuals, albeit at different frequencies. In this context, we believe that raising awareness for the diagnosis and treatment of allergic diseases in elderly patients is necessary.
Competing Interests
The authors had no relevant financial interests to disclose.
Author’s Contributions
Both authors were involved in designing and conducting the study, data collection, analyzing and interpreting the data, preparing the manuscript for publication, and reviewing the manuscript draft. All authors have read and approved the final manuscript
Conflicts of Interest
The authors declare that they have no conflicts of interest.
Funding
None.
REFERENCES
1 De Martinis M, Sirufo MM, Ginaldi L. Allergy and aging: An old/new emerging health issue. Aging Dis. 2017;8(2):162–75. 10.14336/AD.2016.0831
2 Nam JS, Hwang CS, Hong MP, Kim KS. Prevalence and clinical characteristics of allergic rhinitis in the elderly Korean population. Eur Arch Otorhinolaryngol. 2020;277(12):3367–73. 10.1007/s00405-020-06256-5
3 Spiteri K, Broom D, Bekhet AH, de Caro JX, Laventure B, Grafton K. Barriers and motivators of physical activity participation in middle-aged and older-adults–A systematic review. J Aging Phys Act. 2019;27(4):929–44. 10.1123/japa.2018-0343
4 Cardona V, Guilarte M, Luengo O, Labrador-Horrillo M, Sala-Cunill A, Garriga T. Allergic diseases in the elderly. Clin Transl Allergy. 2011;1:11.
5 Yildiz E, Çölkesen F, Arslan Ş, Evcen R, Sadi Aykan F, Kilinç M, et al. Allergic diseases in the elderly population: A single-center experience. Turk J Med Sci. 2021;51(5):2631–40. 10.3906/sag-2104-55
6 Genuneit J, Standl M. Epidemiology of allergy: Natural course and risk factors of allergic diseases. In: Traidl-Hoffmann C, Zuberbier T, Werfel T, editors. Allergic Diseases – From Basic Mechanisms to Comprehensive Management and Prevention [Internet]. Cham: Springer International Publishing; 2022. pp. 21–7. Available from: 10.1007/164_2021_507
7 Sánchez-Borges M, Ansotegui IJ, Baiardini I, Bernstein J, Canonica GW, Ebisawa M, et al. The challenges of chronic urticaria part 1: Epidemiology, immunopathogenesis, comorbidities, quality of life, and management. World Allergy Organ J. 2021;14(6):100533. 10.1016/j.waojou.2021.100533
8 Zuberbier T, Maurer M. Urticaria: Current opinions about etiology, diagnosis and therapy. Acta Derm Venereol. 2007;87(3):196–205. 10.2340/00015555-0240
9 Wilkerson RG. Drug hypersensitivity reactions. Immunol Allergy Clin North Am. 2023;43(3):473–89. 10.1016/j.iac.2022.10.005
10 Patterson RA, Stankewicz HA. Penicillin allergy. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024. Available from: http://www.ncbi.nlm.nih.gov/books/NBK459320/
11 Maurer M, Zuberbier T, Metz M. The classification, pathogenesis, diagnostic workup, and management of urticaria: An update. In: Traidl-Hoffmann C, Zuberbier T, Werfel T, editors. Allergic Diseases – From Basic Mechanisms to Comprehensive Management and Prevention [Internet]. Cham: Springer International Publishing; 2022. pp. 117–33. Available from: 10.1007/164_2021_506
12 Bigby M. Rates of cutaneous reactions to drugs. Arch Dermatol. 2001;137(6):765–70.
13 Zalewska-Janowska A, Spiewak R, Kowalski ML. Cutaneous manifestation of drug allergy and hypersensitivity. Immunol Allergy Clin North Am. 2017;37(1):165–81. 10.1016/j.iac.2016.08.006
14 Siddiqui ZA, Walker A, Pirwani MM, Tahiri M, Syed I. Allergic rhinitis: Diagnosis and management. Br J Hosp Med Lond Engl 2005. 2022;83(2):1–9. 10.12968/hmed.2021.0570
15 Ediger D, Günaydin FE, Erbay M, Şeker Ü. Trends of sensitization to aeroallergens in patients with allergic rhinitis and asthma in the city of Bursa, South Marmara Sea Region of Turkey. Turk J Med Sci. 2020;50(2):330–6. 10.3906/sag-1908-139
16 Sabroe RA. Acute urticaria. Immunol Allergy Clin North Am. 2014;34(1):11–21. 10.1016/j.iac.2013.07.010
17 Antia C, Baquerizo K, Korman A, Bernstein JA, Alikhan A. Urticaria: A comprehensive review: Epidemiology, diagnosis, and work-up. J Am Acad Dermatol. 2018;79(4):599–614. 10.1016/j.jaad.2018.01.020
18 Chiang V, Kan AKC, Saha C, Au EYL, Li PH. Identifying the most at-risk age-group and longitudinal trends of drug allergy labeling amongst 7.3 million individuals in Hong Kong. BMC Med. 2024;22(1):30. 10.1186/s12916-024-03250-0